

Estimating time to ESRD using kidney failure risk equations: results from the African American Study of Kidney Disease and Hypertension (AASK)
- PMID: 25441435
- PMCID: PMC4339439
- DOI: 10.1053/j.ajkd.2014.07.026
Estimating time to ESRD using kidney failure risk equations: results from the African American Study of Kidney Disease and Hypertension (AASK)
Abstract
Background: Planning for renal replacement therapy, such as referral for arteriovenous fistula placement and transplantation, often is guided by level of estimated glomerular filtration rate (eGFR). The use of risk equations might enable more accurate estimation of time to end-stage renal disease (ESRD), thus improving patient care.
Study design: Prospective observational study.
Setting & participants: 1,094 participants in the African American Study of Kidney Disease and Hypertension (AASK) cohort.
Predictor: Age, sex, urine protein-creatinine ratio ≥ 1g/g, APOL1 high-risk status, and 3-year antecedent eGFR decline.
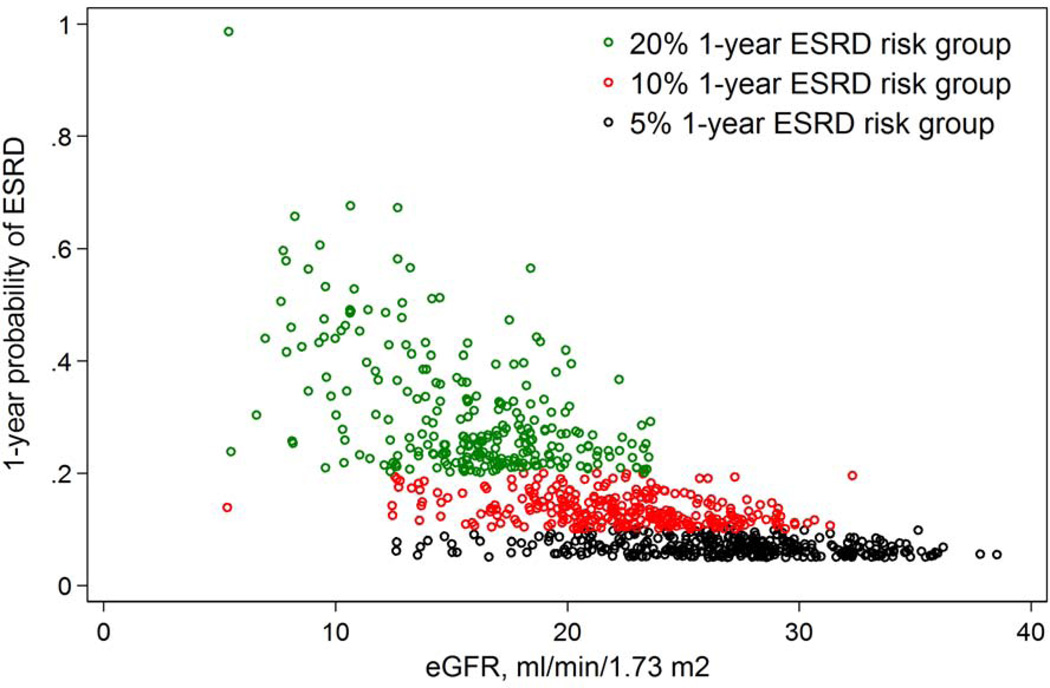
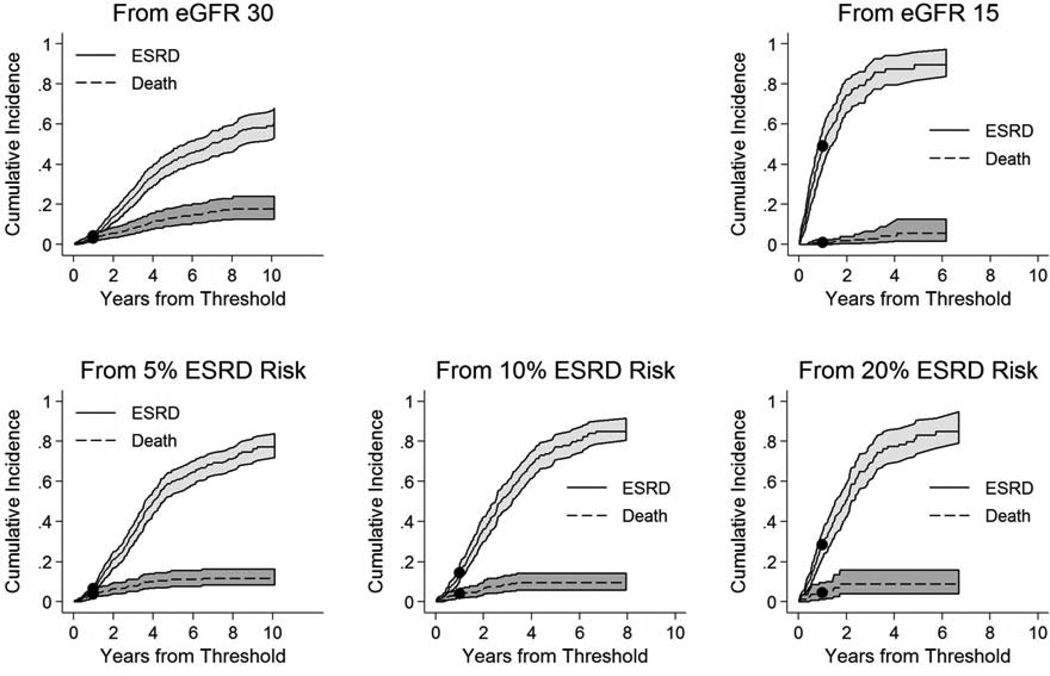
Outcome: Cumulative incidence of ESRD from 5 different starting points: eGFR of 30 and 15mL/min/1.73m(2) and 1-year ESRD risk of 5%, 10%, and 20%, estimated by a published 4-variable kidney failure risk equation.
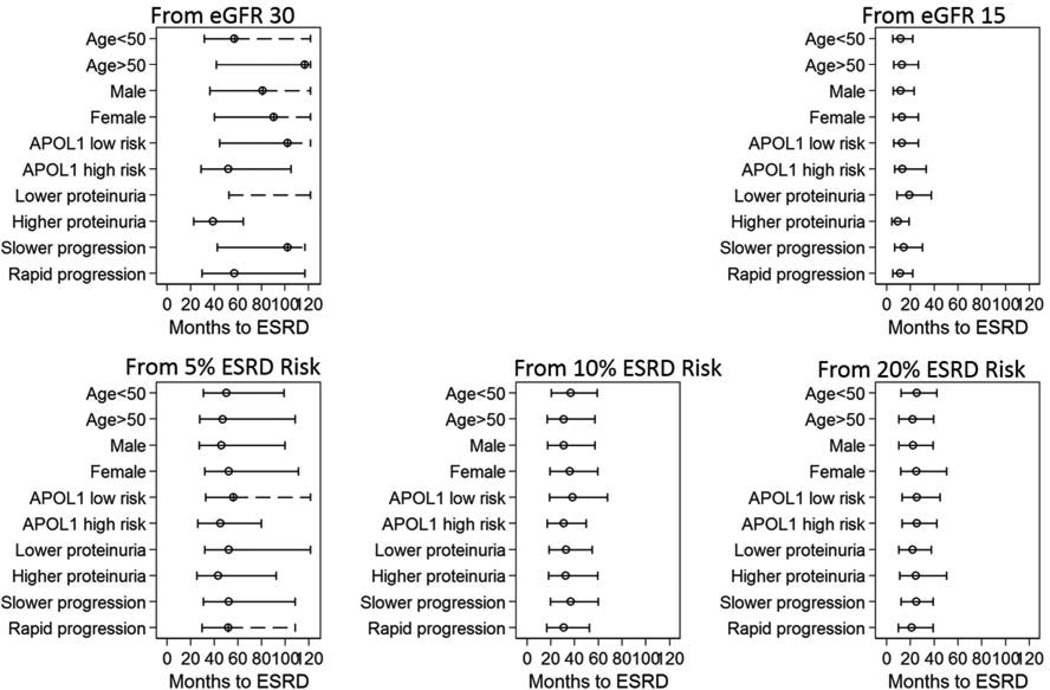
Results: 566 participants developed eGFR of 30mL/min/1.73m(2), 244 developed eGFR of 15mL/min/1.73m(2), and 437, 336, and 259 developed 1-year ESRD risks of 5%, 10%, and 20%, respectively. The 1-year cumulative incidence of ESRD was 4.3% from eGFR of 30mL/min/1.73m(2), 49.0% from eGFR of 15mL/min/1.73m(2), 6.7% from 5% ESRD risk, 15.0% from 10% ESRD risk, and 29% from 20% ESRD risk. From eGFR of 30mL/min/1.73m(2), there were several risk factors that predicted ESRD risk. From eGFR of 15mL/min/1.73m(2), only level of proteinuria did; median time to ESRD was 9 and 19 months in those with higher and lower proteinuria, respectively. Median times were less variable from corresponding ESRD risk thresholds. For example, median times to ESRD from 20% ESRD risk were 22 and 25 months among those with higher and lower proteinuria, respectively.
Limitations: Relatively homogeneous population of African Americans with hypertensive kidney disease.
Conclusions: Results of the present study suggest the potential benefit of incorporating kidney failure risk equations into clinical care, with selection of a specific threshold guided by its intended use.
Keywords: African American Study of Kidney Disease and Hypertension (AASK); End-stage renal disease (ESRD); clinical decision making; disease progression; disease trajectory; estimated glomerular filtration rate (eGFR); hypertensive kidney disease; kidney failure risk equations; prognosis; proteinuria; risk.
Copyright © 2015 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Use of the Kidney Failure Risk Equation to reduce uncertainty in predicting time to ESRD.Am J Kidney Dis. 2015 Mar;65(3):369-71. doi: 10.1053/j.ajkd.2015.01.002. Am J Kidney Dis. 2015. PMID: 25704041 No abstract available.
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. The New England journal of medicine. 2004;351:1296–1305. - PubMed
-
- Ishani A, Grandits GA, Grimm RH, et al. Association of single measurements of dipstick proteinuria, estimated glomerular filtration rate, and hematocrit with 25-year incidence of end-stage renal disease in the multiple risk factor intervention trial. Journal of the American Society of Nephrology : JASN. 2006;17:1444–1452. - PubMed
-
- Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Archives of Internal Medicine. 2004;164:659–663. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
