

Receipt of diabetes preventive services differs by insurance status at visit
- PMID: 25442228
- PMCID: PMC4301980
- DOI: 10.1016/j.amepre.2014.08.035
Receipt of diabetes preventive services differs by insurance status at visit
Abstract
Background: Lack of insurance is associated with suboptimal receipt of diabetes preventive care. One known reason for this is an access barrier to obtaining healthcare visits; however, little is known about whether insurance status is associated with differential rates of receipt of diabetes care during visits.
Purpose: To examine the association between health insurance and receipt of diabetes preventive care during an office visit.
Methods: This retrospective cohort study used electronic health record and Medicaid data from 38 Oregon community health centers. Logistic regression was used to test the association between insurance and receipt of four diabetes services during an office visit among patients who were continuously uninsured (n=1,117); continuously insured (n=1,466); and discontinuously insured (n=336) in 2006-2007. Generalized estimating equations were used to account for within-patient correlation. Data were analyzed in 2013.
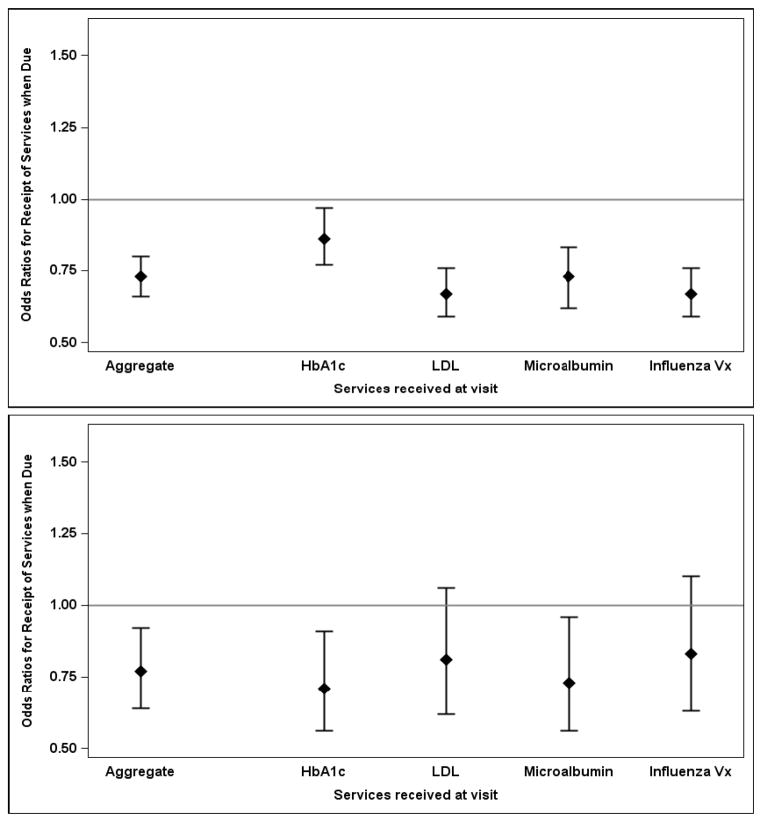
Results: Overall, continuously uninsured patients had lower odds of receiving services at visits when due, compared to those who were continuously insured (AOR=0.73, 95% CI=0.66, 0.80). Among the discontinuously insured, being uninsured at a visit was associated with lower odds of receipt of services due at that visit (AOR=0.77, 95% CI=0.64, 0.92) than being insured at a visit.
Conclusions: Lack of insurance is associated with a lower probability of receiving recommended services that are due during a clinic visit. Thus, the association between being uninsured and receiving fewer preventive services may not be completely mediated by access to clinic visits.
Copyright © 2015 American Journal of Preventive Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no potential conflicts of interest to declare.
Figures
References
-
- Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med. 2003;348(5):383–93. - PubMed
-
- Harris R, Donahue K, Rathore SS, Frame P, Woolf SH, Lohr KN. Screening adults for type 2 diabetes: a review of the evidence for the U.S. Preventive Services Task Force. Ann Internal Med. 2003;138(3):215–29. - PubMed
-
- US Department of Health & Human Services. AHRQ Publication No 12-0005. Rockville, MD: Agency for Healthcare Research and Quality; 2012. National Healthcare Quality Report, 2011.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
