

Bridge to removal: a paradigm shift for left ventricular assist device therapy
- PMID: 25442985
- PMCID: PMC4283551
- DOI: 10.1016/j.athoracsur.2014.07.061
Bridge to removal: a paradigm shift for left ventricular assist device therapy
Abstract
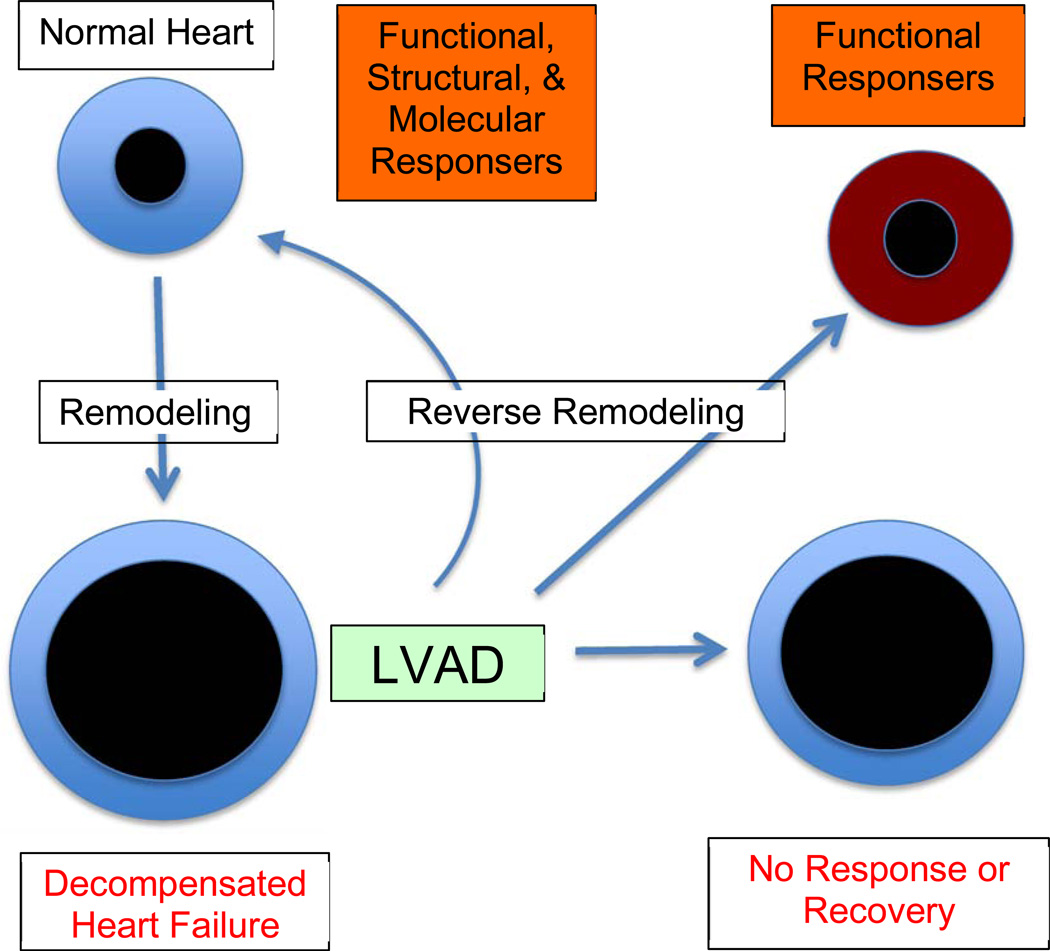
Ventricular assist devices have become standard therapy for patients with advanced heart failure either as a bridge to transplantation or destination therapy. Despite the functional and biologic evidence of reverse cardiac remodeling, few patients actually proceed to myocardial recovery, and even fewer to the point of having their device explanted. An enhanced understanding of the biology and care of the mechanically supported patient has redirected focus on the possibility of using ventricular assist devices as a bridge to myocardial recovery and removal. Herein, we review the current issues and approaches to transforming myocardial recovery to a practical reality.
Copyright © 2015 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Miller LW, Pagani FD, Russell SD, et al. Use of a continuous-flow device in patients awaiting heart transplantation. N Engl J Med. 2007;357(9):885–896. - PubMed
-
- Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. 2001;345(20):1435–1443. - PubMed
-
- Slaughter MS, Rogers JG, Milano CA, et al. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med. 2009;361(23):2241–2251. - PubMed
-
- Birks EJ, George RS, Firouzi A, et al. Long-term outcomes of patients bridged to recovery versus patients bridged to transplantation. J Thorac Cardiovasc Surg. 2012;144(1):190–196. - PubMed
-
- Birks EJ, George RS, Hedger M, et al. Reversal of severe heart failure with a continuous-flow left ventricular assist device and pharmacological therapy: A prospective study. Circulation. 2011;123(4):381–390. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
