

Hospital readmission is associated with poor survival after esophagectomy for esophageal cancer
- PMID: 25442987
- PMCID: PMC4282960
- DOI: 10.1016/j.athoracsur.2014.07.052
Hospital readmission is associated with poor survival after esophagectomy for esophageal cancer
Abstract
Background: Hospital readmissions are costly and associated with inferior patient outcomes. There is limited knowledge related to readmissions after esophagectomy for malignancy. Our aim was to determine the impact on survival of readmission after esophagectomy.
Methods: This cohort study utilizes Surveillance, Epidemiology, and End Results-Medicare data (2002 to 2009). Survival, length of stay, 30-day readmissions, and discharge disposition were determined. Multivariate logistic regression models were created to examine risk factors associated with readmission.
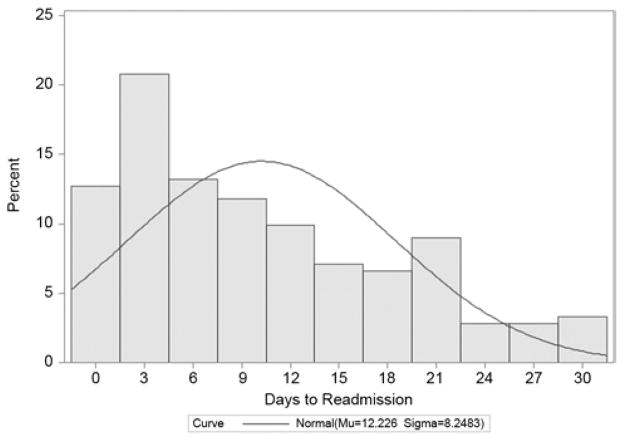
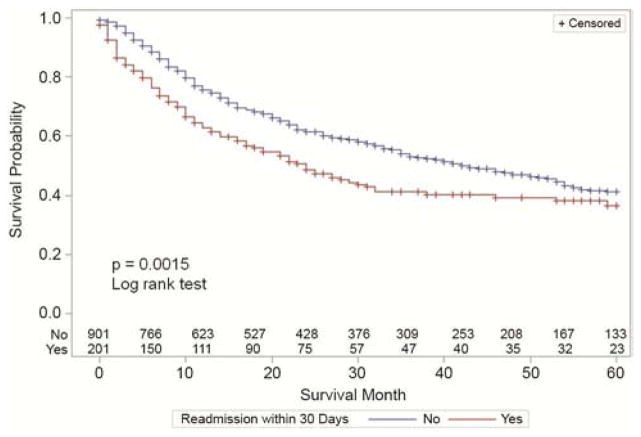
Results: In all, 1,744 patients with esophageal cancer underwent esophagectomy: 80% of patients (1,390) were male, and mean age was 73 years; 71.8% of tumors (1,251) were adenocarcinomas, and 72.5% (1,265) were distal esophageal tumors; 38% of patients (667) received induction therapy. Operative approach was transthoracic in 52.6% of patients (918) and transhiatal in 37.4% (653), and required complex reconstruction (intestinal interposition) in 9.9% (173). Stage distribution was as follows: stage I, 35.3% (616); stage II, 32.5% (566); stage III, 27.9% (487); and stage IV, 2.3% (40). Median length of stay was 13 days, hospital mortality was 9.3% (158 patients), and 30-day readmission rate was 18.6% (212 of 1,139 home discharges); 25.4% of patients (443) were discharged to institutional care facilities. Overall survival was significantly worse for patients who were readmitted (p < 0.0001, log rank test). Risk factors for readmission were comorbidity score of 3+, urgent admission, and urban residence.
Conclusions: Hospital readmissions after esophagectomy for cancer occur frequently and are associated with worse survival. Improved identification of patients at risk for readmission after esophagectomy can inform patient selection, discharge planning, and outpatient monitoring. Optimization of such practices may lead to improved outcomes at reduced cost.
Copyright © 2015 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–28. - PubMed
-
- Schneider EB, Hyder O, Brooke BS, et al. Patient readmission and mortality after colorectal surgery for colon cancer: impact of length of stay relative to other clinical factors. J Am Coll Surg. 2012;214(4):390–398. - PubMed
-
- [Accessed January 12, 2014];CMS Readmissions Reductions Program. Available at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpati....
-
- Maniar HS, Bell JM, Moon MR, et al. Prospective evaluation of patients readmitted after cardiac surgery: Analysis of outcomes and identification of risk factors. J Thorac Cardiovasc Surg. 2013 [Epub] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
