

Clinical implications of chronic heart failure phenotypes defined by cluster analysis
- PMID: 25443696
- PMCID: PMC4254424
- DOI: 10.1016/j.jacc.2014.07.979
Clinical implications of chronic heart failure phenotypes defined by cluster analysis
Abstract
Background: Classification of chronic heart failure (HF) is on the basis of criteria that may not adequately capture disease heterogeneity. Improved phenotyping may help inform research and therapeutic strategies.
Objectives: This study used cluster analysis to explore clinical phenotypes in chronic HF patients.
Methods: A cluster analysis was performed on 45 baseline clinical variables from 1,619 participants in the HF-ACTION (Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training) study, which evaluated exercise training versus usual care in chronic systolic HF. An association between identified clusters and clinical outcomes was assessed using Cox proportional hazards modeling. Differential associations between clinical outcomes and exercise testing were examined using interaction testing.
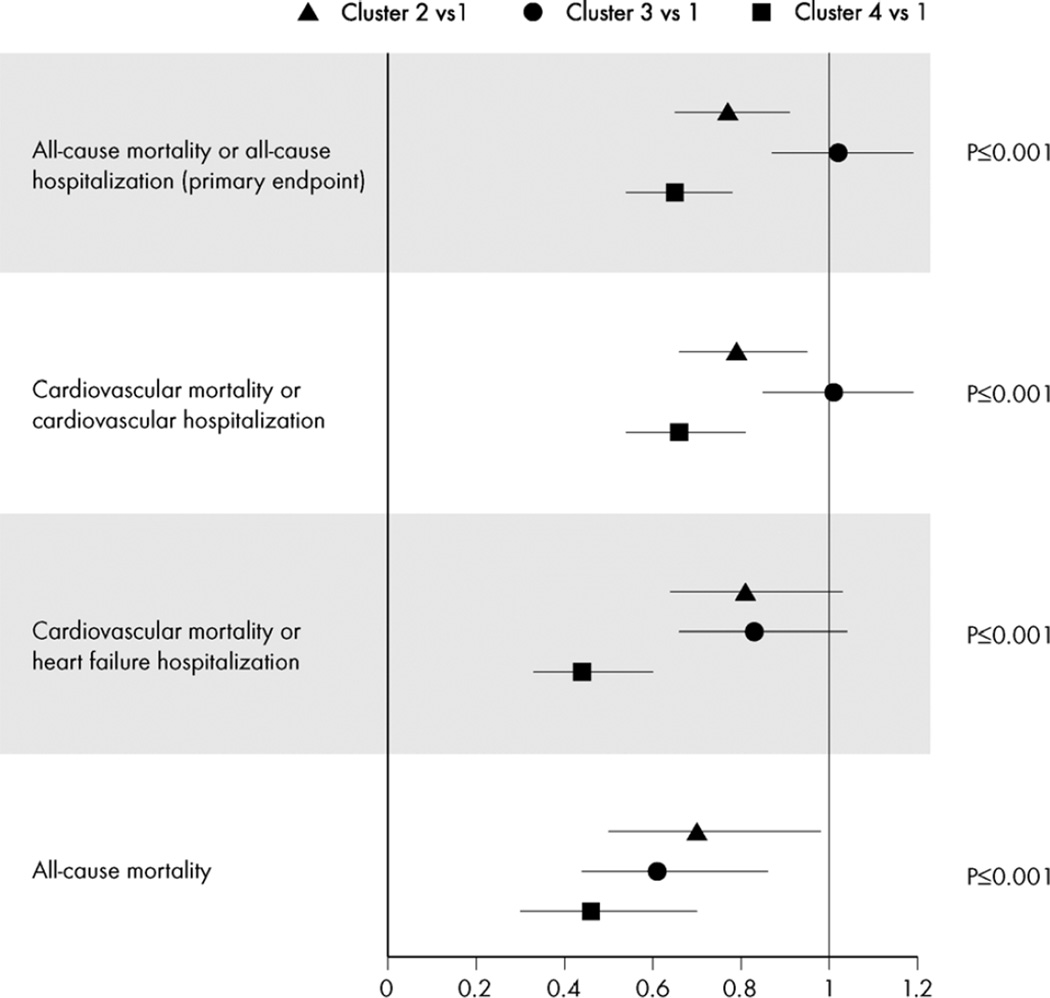
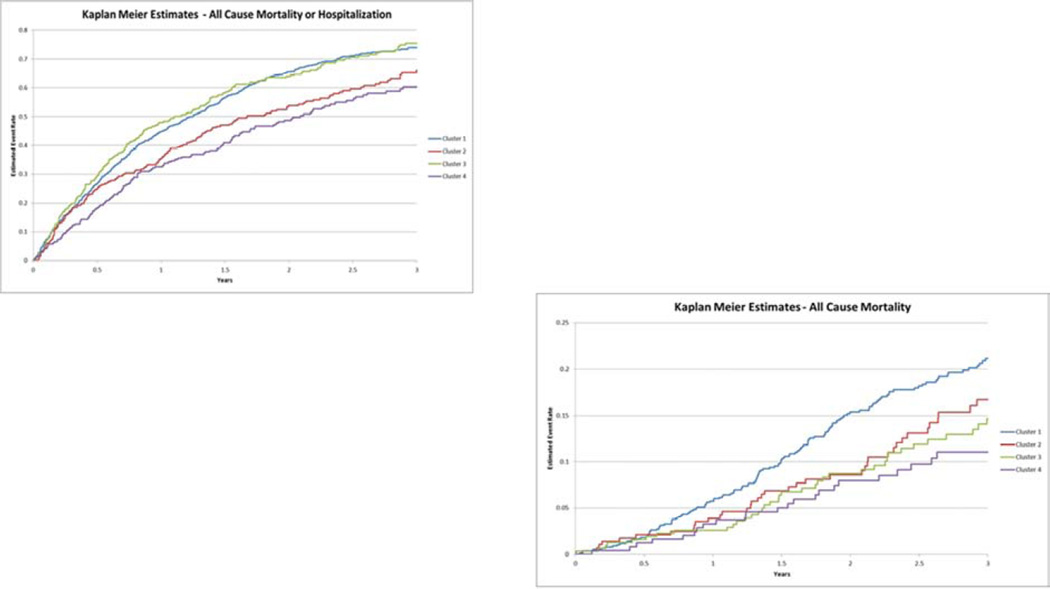
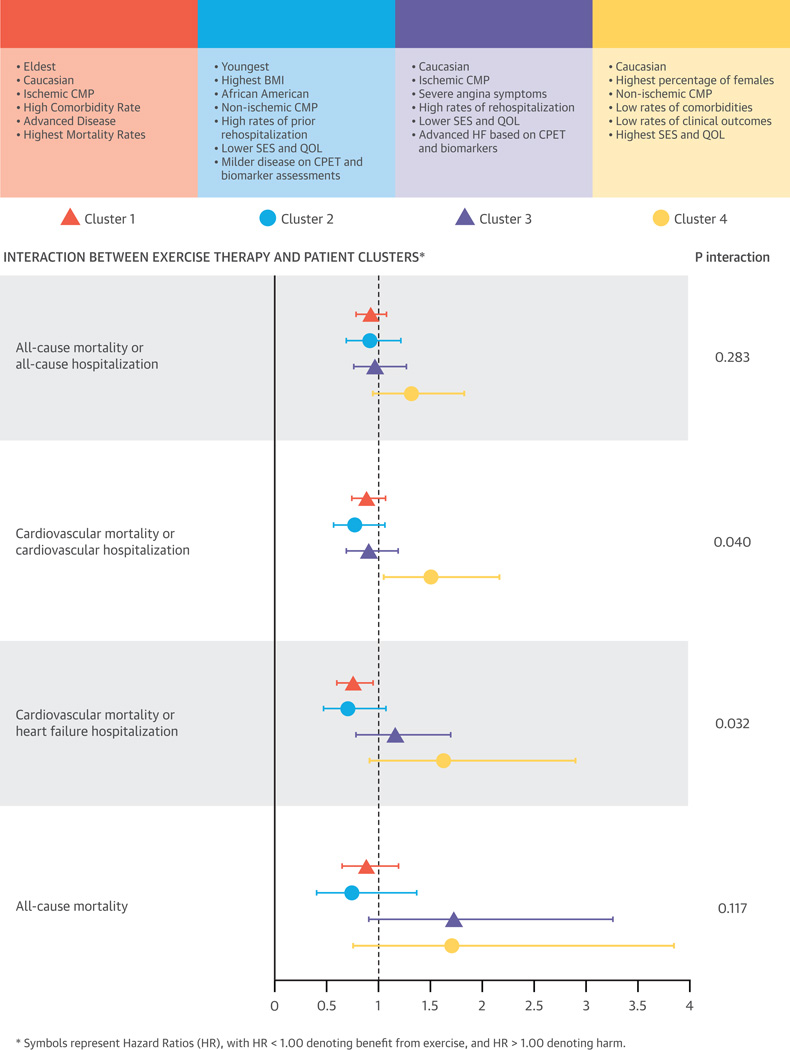
Results: Four clusters were identified (ranging from 248 to 773 patients in each), in which patients varied considerably among measures of age, sex, race, symptoms, comorbidities, HF etiology, socioeconomic status, quality of life, cardiopulmonary exercise testing parameters, and biomarker levels. Differential associations were observed for hospitalization and mortality risks between and within clusters. Compared with cluster 1, risk of all-cause mortality and/or all-cause hospitalization ranged from 0.65 (95% confidence interval [95% CI]: 0.54 to 0.78) for cluster 4 to 1.02 (95% CI: 0.87 to 1.19) for cluster 3. However, for all-cause mortality, cluster 3 had a disproportionately lower risk of 0.61 (95% CI: 0.44 to 0.86). Evidence suggested differential effects of exercise treatment on changes in peak oxygen consumption and clinical outcomes between clusters (p for interaction <0.04).
Conclusions: Cluster analysis of clinical variables identified 4 distinct phenotypes of chronic HF. Our findings underscore the high degree of disease heterogeneity that exists within chronic HF patients and the need for improved phenotyping of the syndrome. (Exercise Training Program to Improve Clinical Outcomes in Individuals With Congestive Heart Failure; NCT00047437).
Keywords: mortality; prognosis; rehospitalization; socioeconomic.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The heterogeneity of heart failure: will enhanced phenotyping be necessary for future clinical trial success?J Am Coll Cardiol. 2014 Oct 28;64(17):1775-6. doi: 10.1016/j.jacc.2014.07.978. Epub 2014 Oct 21. J Am Coll Cardiol. 2014. PMID: 25443697 No abstract available.
-
Systems biology and clinical phenotypes of heart failure syndrome.J Am Coll Cardiol. 2015 Mar 31;65(12):1269-1270. doi: 10.1016/j.jacc.2014.12.051. J Am Coll Cardiol. 2015. PMID: 25814239 No abstract available.
-
Reply: applying cluster analysis to data of previously published chronic heart failure trials.J Am Coll Cardiol. 2015 Mar 31;65(12):1270. doi: 10.1016/j.jacc.2014.11.069. J Am Coll Cardiol. 2015. PMID: 25814241 No abstract available.
References
-
- McMurray JJ, Adamopoulos S, Anker SD, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787–1847. - PubMed
-
- Braunwald E. Heart Failure. JACC Heart Fail. 2013;1:1–20. - PubMed
-
- De Keulenaer GW, Brutsaert DL. Systolic and diastolic heart failure: different phenotypes of the same disease? Eur J Heart Fail. 2007;9:136–143. - PubMed
-
- Dickstein K, Cohen-Solal A, Filippatos G, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the diagnosis and treatment of acute and chronic heart failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM) Eur J Heart Fail. 2008;10:933–989. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
