

Left ventricular noncompaction: a distinct cardiomyopathy or a trait shared by different cardiac diseases?
- PMID: 25443708
- PMCID: PMC10352990
- DOI: 10.1016/j.jacc.2014.08.030
Left ventricular noncompaction: a distinct cardiomyopathy or a trait shared by different cardiac diseases?
Abstract
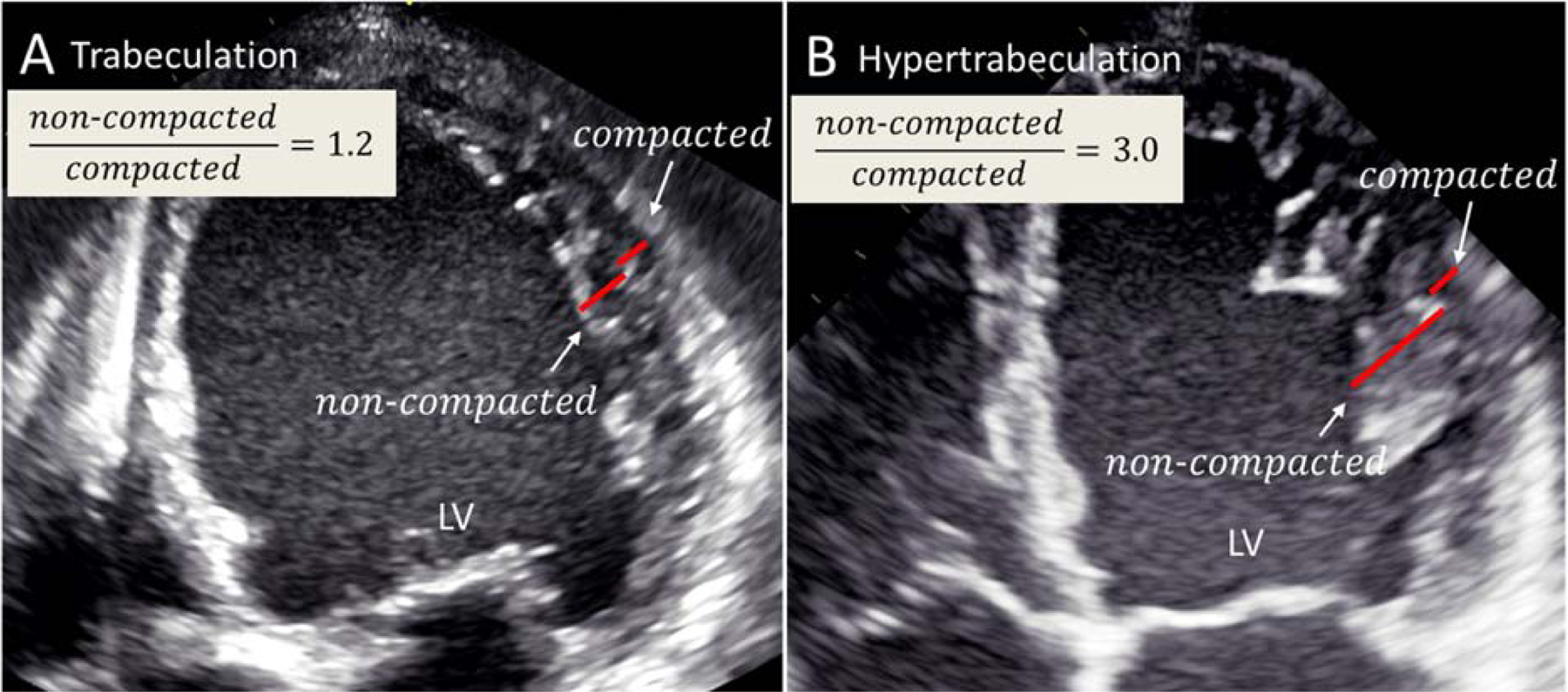
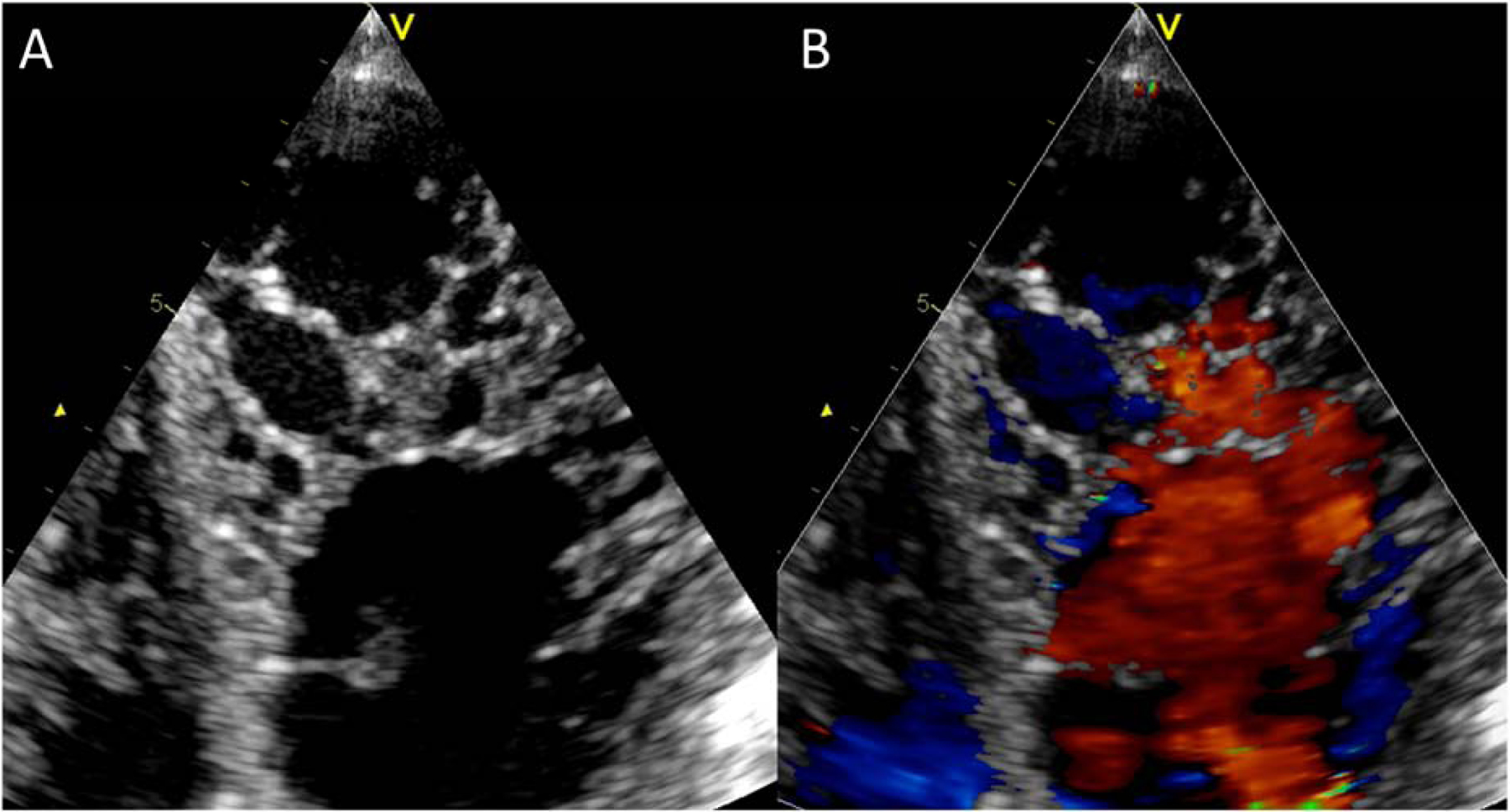
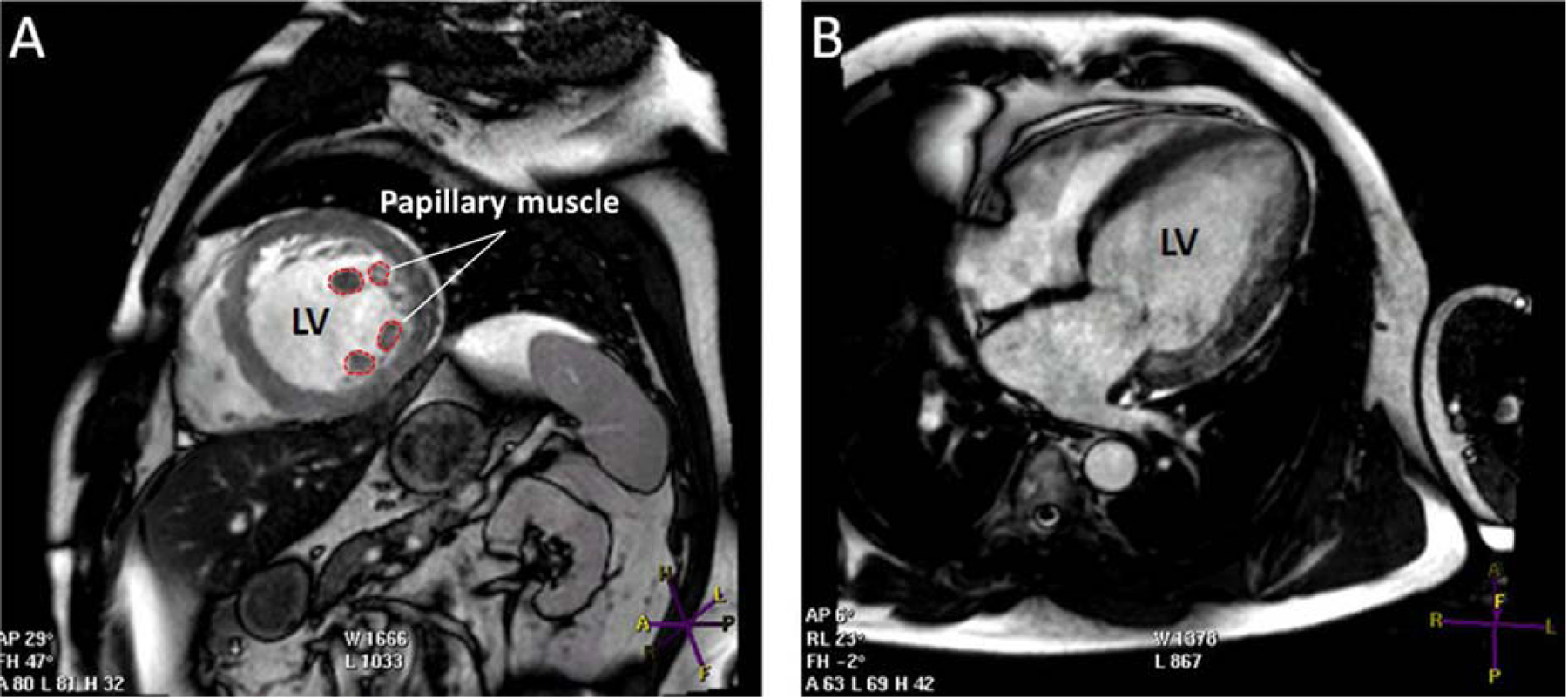
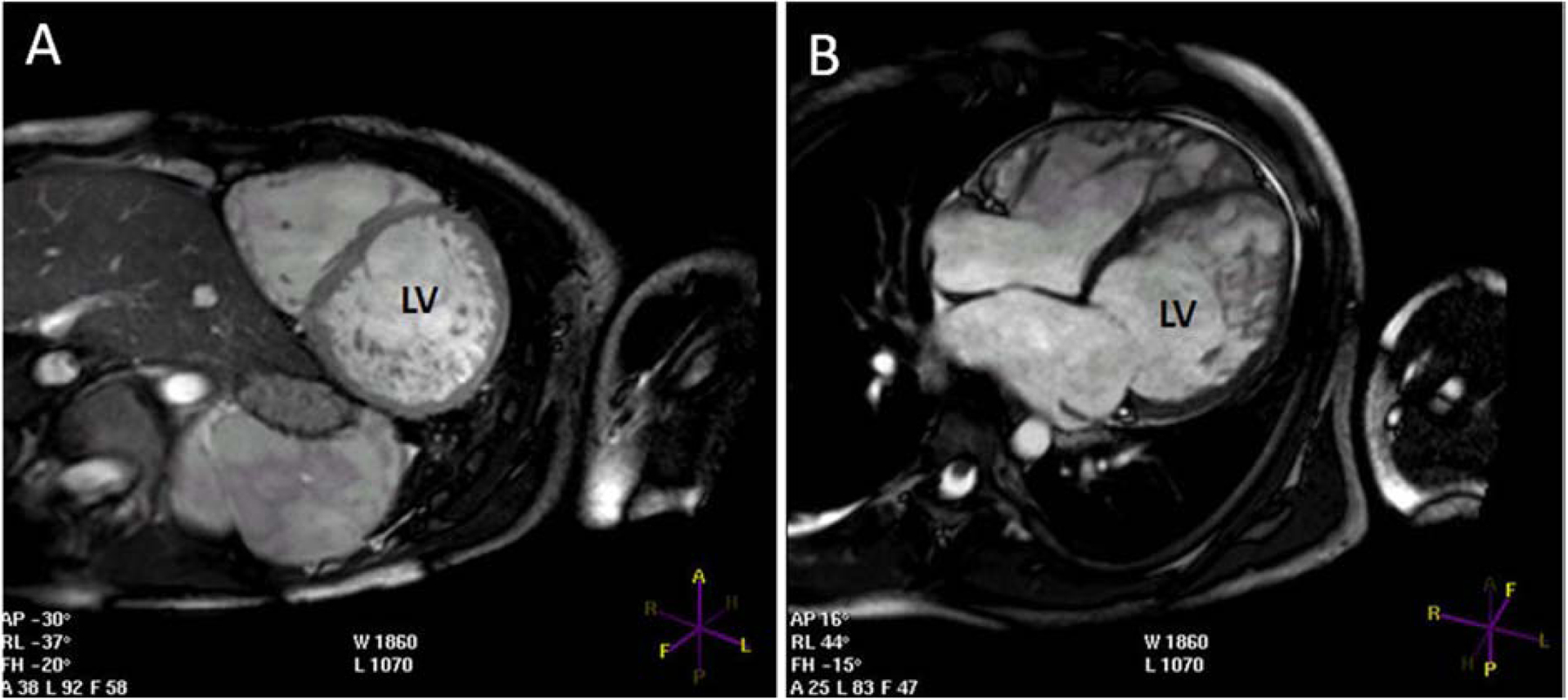
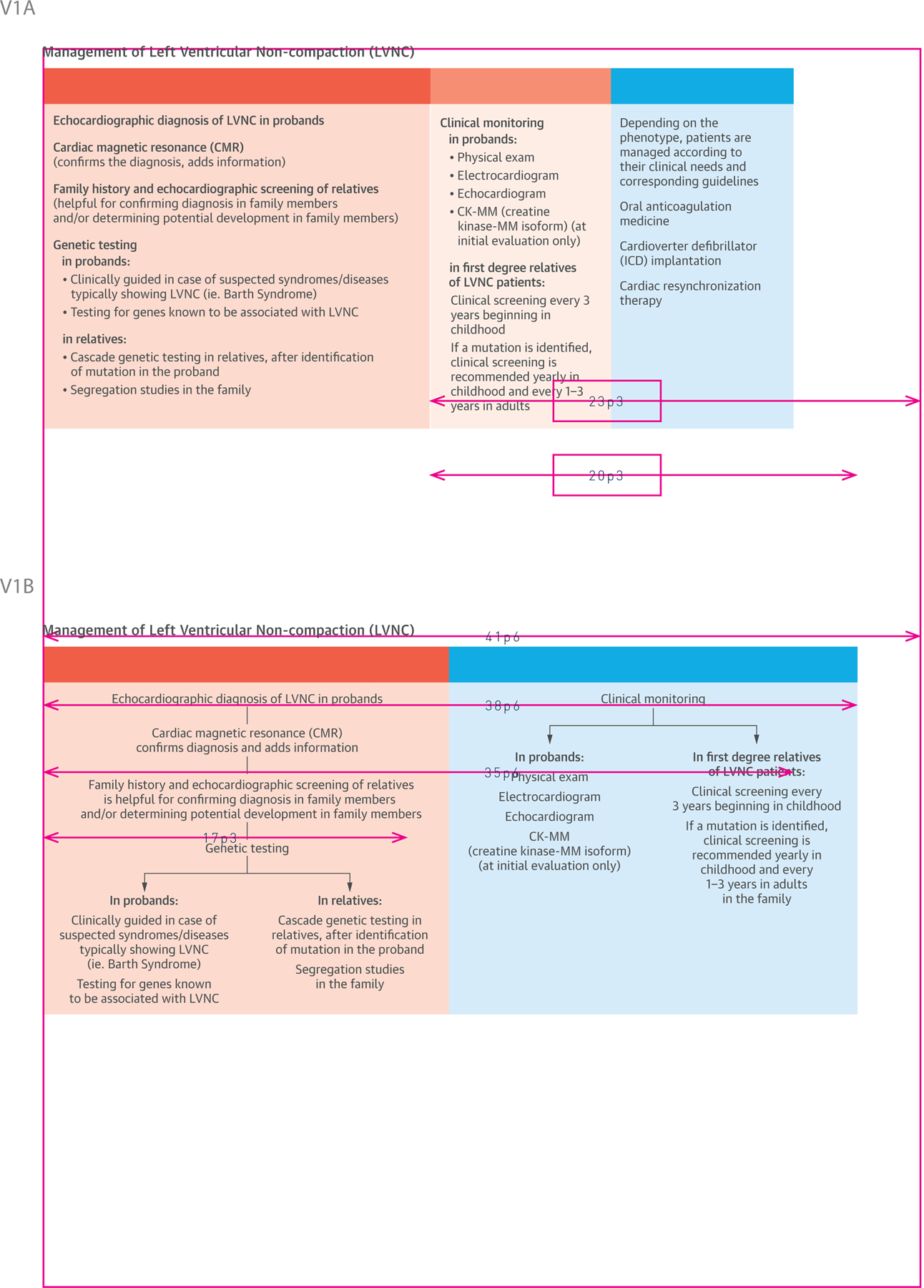
Whether left ventricular noncompaction (LVNC) is a distinct cardiomyopathy or a morphologic trait shared by different cardiomyopathies remains controversial. Current guidelines from professional organizations recommend different strategies for diagnosing and treating patients with LVNC. This state-of-the-art review discusses new insights into the basic mechanisms leading to LVNC, its clinical manifestations, treatment modalities, anatomy and pathology, embryology, genetics, epidemiology, and imaging. Three markers currently define LVNC: prominent left ventricular trabeculae, deep intertrabecular recesses, and a thin compacted layer. Although new genetic data from mice and humans supports LVNC as a distinct cardiomyopathy, evidence for LVNC as a shared morphological trait is not ruled out. Criteria supporting LVNC as a shared morphological trait may depend on consensus guidelines from the multiple professional organizations. Enhanced imaging and increased use of genetics are both predicted to significantly impact our overall understanding of the basic mechanisms causing LVNC and its optimal management.
Keywords: compacted; epidemiology; genetics; imaging; pathology; trabeculae.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The importance of the cardiac cycle in the imaging criteria for left ventricular noncompaction.J Am Coll Cardiol. 2015 Apr 7;65(13):1382-1383. doi: 10.1016/j.jacc.2014.11.072. J Am Coll Cardiol. 2015. PMID: 25835456 No abstract available.
-
Reply: The importance of cardiac cycle in the imaging criteria for left ventricular noncompaction.J Am Coll Cardiol. 2015 Apr 7;65(13):1383-1384. doi: 10.1016/j.jacc.2014.12.054. J Am Coll Cardiol. 2015. PMID: 25835457 No abstract available.
References
-
- Maron BJ, Towbin JA, Thiene G, et al. ; American Heart Association; Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; Council on Epidemiology and Prevention. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 2006;113:1807–16. - PubMed
-
- Elliott P, Andersson B, Arbustini E, et al. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2008;29:270–6. - PubMed
-
- The Fuster V. 3 pathways of translational medicine: an evolution to a call-and-response method. J Am Coll Cardiol 2014;64:223–5. - PubMed
-
- Zaragoza MV, Arbustini E, Narula J. Noncompaction of the left ventricle: primary cardiomyopathy with an elusive genetic etiology. Curr Opinion Pediatrics 2007;19:619–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
