

Prognostic value of elevated levels of intestinal microbe-generated metabolite trimethylamine-N-oxide in patients with heart failure: refining the gut hypothesis
- PMID: 25444145
- PMCID: PMC4254529
- DOI: 10.1016/j.jacc.2014.02.617
Prognostic value of elevated levels of intestinal microbe-generated metabolite trimethylamine-N-oxide in patients with heart failure: refining the gut hypothesis
Abstract
Background: Altered intestinal function is prevalent in patients with heart failure (HF), but its role in adverse outcomes is unclear.
Objectives: This study investigated the potential pathophysiological contributions of intestinal microbiota in HF.
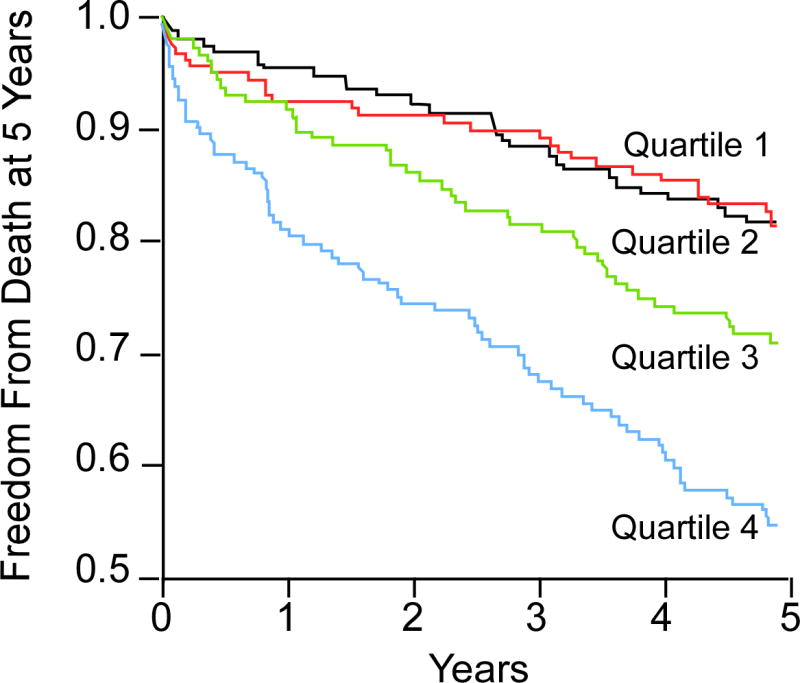
Methods: We examined the relationship between fasting plasma trimethylamine-N-oxide (TMAO) and all-cause mortality over a 5-year follow-up in 720 patients with stable HF.
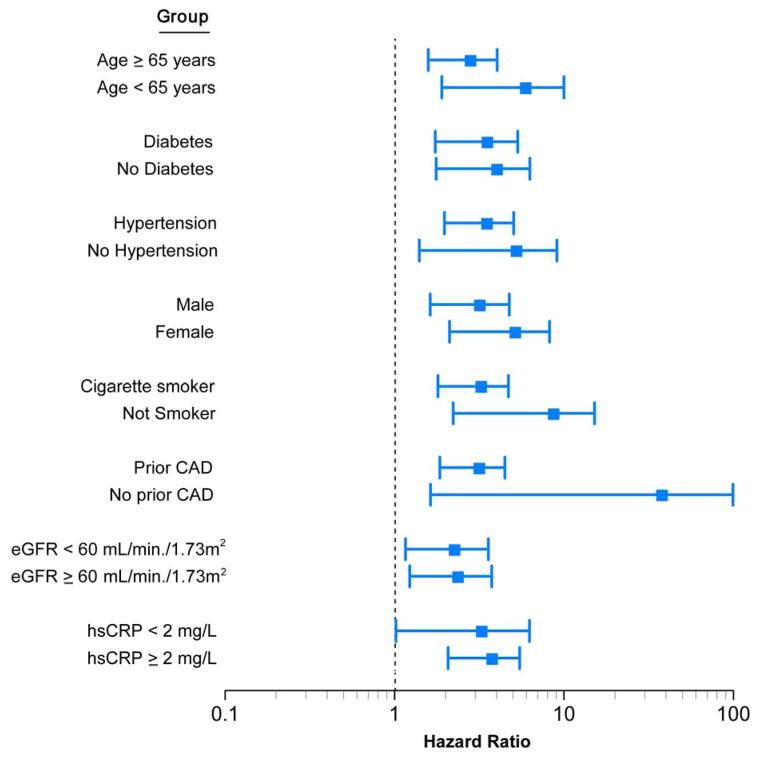
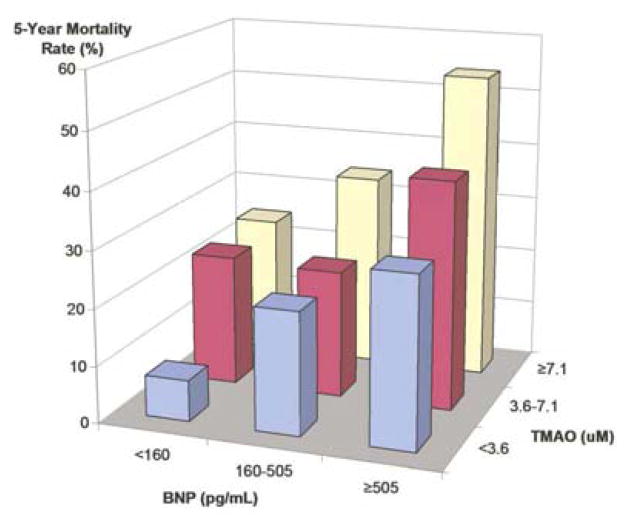
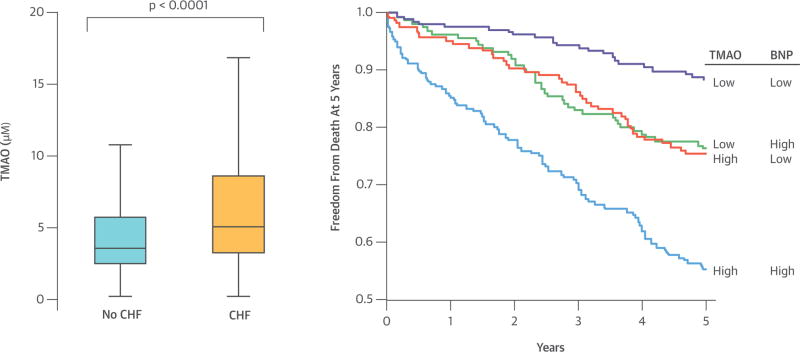
Results: The median TMAO level was 5.0 μM, which was higher than in subjects without HF (3.5 μM; p < 0.001). There was modest but significant correlation between TMAO concentrations and B-type natriuretic peptide (BNP) levels (r = 0.23; p < 0.001). Higher plasma TMAO levels were associated with a 3.4-fold increased mortality risk. Following adjustments for traditional risk factors and BNP levels, elevated TMAO levels remained predictive of 5-year mortality risk (hazard ratio [HR]: 2.2; 95% CI: 1.42 to 3.43; p < 0.001), as well as following the addition of estimated glomerular filtration rate to the model (HR: 1.75; 95% CI: 1.07 to 2.86; p < 0.001).
Conclusions: High TMAO levels were observed in patients with HF, and elevated TMAO levels portended higher long-term mortality risk independent of traditional risk factors and cardiorenal indexes.
Keywords: C-reactive protein; TMAO; cardiorenal; intestinal microbiota; mortality.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Gut feelings about heart failure.J Am Coll Cardiol. 2014 Nov 4;64(18):1915-6. doi: 10.1016/j.jacc.2014.04.088. Epub 2014 Oct 27. J Am Coll Cardiol. 2014. PMID: 25444146 No abstract available.
References
-
- Krack A, Sharma R, Figulla HR, Anker SD. The importance of the gastrointestinal system in the pathogenesis of heart failure. Eur Heart J. 2005;26:2368–74. - PubMed
-
- Verbrugge FH, Dupont M, Steels P, et al. Abdominal contributions to cardiorenal dysfunction in congestive heart failure. J Am Coll Cardiol. 2013;62:485–95. - PubMed
-
- Rauchhaus M, Anker SD. Plasma concentrations of bacterial lipopolysaccharide: a marker of infection or inflammation? J Am Coll Cardiol. 2000;36:656–7. - PubMed
-
- Sandek A, Bauditz J, Swidsinski A, et al. Altered intestinal function in patients with chronic heart failure. J Am Coll Cardiol. 2007;50:1561–9. - PubMed
-
- Vasko MR, Cartwright DB, Knochel JP, Nixon JV, Brater DC. Furosemide absorption altered in decompensated congestive heart failure. Ann Intern Med. 1985;102:314–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01HL103866/HL/NHLBI NIH HHS/United States
- UL1TR 000439/TR/NCATS NIH HHS/United States
- R01 HL103931/HL/NHLBI NIH HHS/United States
- R01 HL103866/HL/NHLBI NIH HHS/United States
- P01 HL076491/HL/NHLBI NIH HHS/United States
- P20HL113452/HL/NHLBI NIH HHS/United States
- P20 HL113452/HL/NHLBI NIH HHS/United States
- P01HL098055/HL/NHLBI NIH HHS/United States
- R01HL103931/HL/NHLBI NIH HHS/United States
- P01 HL098055/HL/NHLBI NIH HHS/United States
- P01HL076491/HL/NHLBI NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
