

Axillary reverse mapping: five-year experience
- PMID: 25444319
- PMCID: PMC4354953
- DOI: 10.1016/j.surg.2014.05.011
Axillary reverse mapping: five-year experience
Abstract
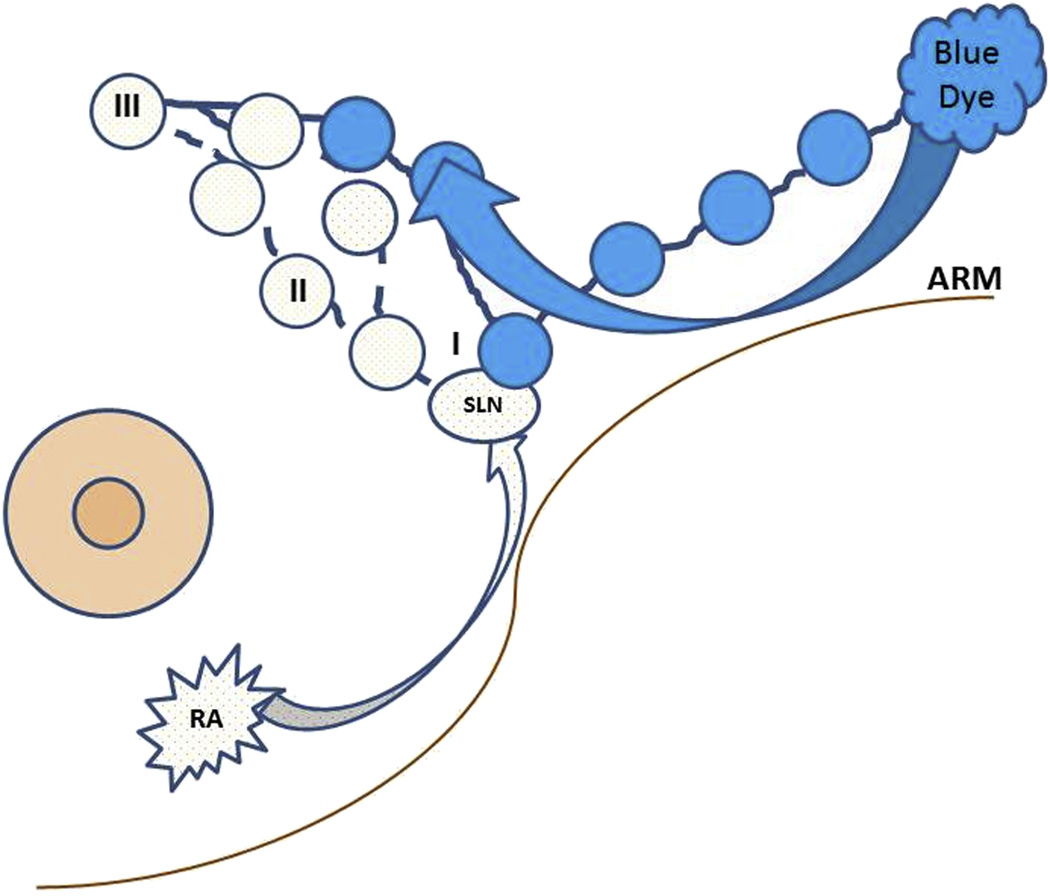
Background: We hypothesize that mapping the lymphatic drainage of the arm with blue dye (axillary reverse mapping [ARM]) during axillary lymphadenectomy decreases the likelihood of disruption of lymphatics and subsequent lymphedema.
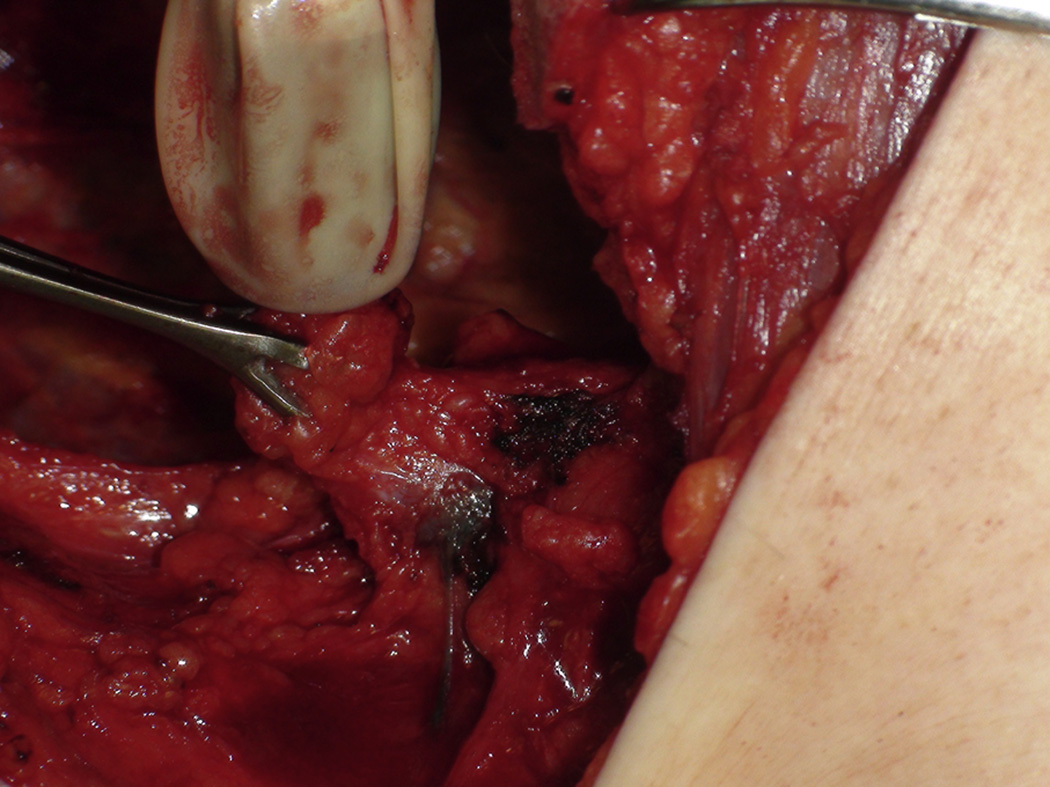
Methods: This institutional review board-approved study involved 360 patients undergoing sentinel lymph node biopsy (SLNB) and/or axillary lymph node dissection (ALND) from May 2006 to October 2011. Technetium sulfur colloid (4 mL) was injected subareolarly, and 5 mL of blue dye was injected subcutaneously in the volar surface ipsilateral upper extremity (ARM). Data were collected on variations in lymphatic drainage, successful identification and protection of arm lymphatics, crossover, and occurrence of lymphedema.
Results: A group of 360 patients underwent SLNB and/or ALND, 348 of whom underwent a SLNB. Of those, 237 (68.1%) had a SLNB only, and 111 (31.9%) went on to an ALND owing to a positive axilla. An additional 12 of 360 (3.3%) axilla had ALND owing to a clinically positive axilla/preoperative core needle biopsy. In 96% of patients with SLNB (334/348), breast SLNs were hot but not blue; crossover (SLN hot and blue) was seen in 14 of 348 patients (4%). Blue lymphatics were identified in 80 of 237 SLN incisions (33.7%) and in 93 of 123 ALND (75.4%). Average follow-up was 12 months (range, 3-48) and resulted in a SLNB lymphedema rate of 1.7% (4/237) and ALND of 2.4% (3/123).
Conclusion: ARM identified substantial lymphatic variations draining the upper extremities and facilitated preservation. Metastases in ARM-identified lymph nodes were acceptably low, indicating that ARM is safe. ARM added to present-day ALND and SLNB may be useful to lesser rates of lymphedema.
Copyright © 2014. Published by Elsevier Inc.
Figures
Similar articles
-
The Feasibility and Oncological Safety of Axillary Reverse Mapping in Patients with Breast Cancer: A Systematic Review and Meta-Analysis of Prospective Studies.PLoS One. 2016 Feb 26;11(2):e0150285. doi: 10.1371/journal.pone.0150285. eCollection 2016. PLoS One. 2016. PMID: 26919589 Free PMC article.
-
Axillary reverse mapping (ARM): a new concept to identify and enhance lymphatic preservation.Ann Surg Oncol. 2007 Jun;14(6):1890-5. doi: 10.1245/s10434-007-9412-x. Epub 2007 May 4. Ann Surg Oncol. 2007. PMID: 17479341
-
Does Axillary Reverse Mapping Prevent Lymphedema After Lymphadenectomy?Ann Surg. 2017 May;265(5):987-992. doi: 10.1097/SLA.0000000000001778. Ann Surg. 2017. PMID: 27163955 Clinical Trial.
-
Axillary reverse mapping: mapping and preserving arm lymphatics may be important in preventing lymphedema during sentinel lymph node biopsy.J Am Coll Surg. 2008 May;206(5):1038-42; discussion 1042-4. doi: 10.1016/j.jamcollsurg.2007.12.022. Epub 2008 Mar 3. J Am Coll Surg. 2008. PMID: 18471751 Clinical Trial.
-
Axillary reverse mapping (ARM): where to go.Breast Cancer. 2019 Jan;26(1):1-10. doi: 10.1007/s12282-018-0886-0. Epub 2018 Jun 30. Breast Cancer. 2019. PMID: 29961238 Review.
Cited by
-
Prevention of Breast Cancer-Related Lymphedema: An Up-to-Date Systematic Review of Different Surgical Approaches.J Clin Med. 2024 Jan 18;13(2):555. doi: 10.3390/jcm13020555. J Clin Med. 2024. PMID: 38256688 Free PMC article. Review.
-
The Use of Wearable Activity Monitors to Measure Upper Limb Physical Activity After Axillary Lymph Node Dissection and Sentinel Lymph Node Biopsy.Ann Surg Oncol. 2023 Nov;30(12):7036-7045. doi: 10.1245/s10434-023-13966-7. Epub 2023 Jul 28. Ann Surg Oncol. 2023. PMID: 37507555 Free PMC article.
-
Reverse Axillary Mapping in Breast Cancer Using Blue Dye: A Tertiary Setup Experience.Cureus. 2021 Oct 7;13(10):e18576. doi: 10.7759/cureus.18576. eCollection 2021 Oct. Cureus. 2021. PMID: 34760419 Free PMC article.
-
Five-Year Breast Surgeon Experience in LYMPHA at Time of ALND for Treatment of Clinical T1-4N1-3M0 Breast Cancer.Ann Surg Oncol. 2021 Oct;28(10):5775-5787. doi: 10.1245/s10434-021-10551-8. Epub 2021 Aug 7. Ann Surg Oncol. 2021. PMID: 34365563 Free PMC article.
-
The Feasibility and Oncological Safety of Axillary Reverse Mapping in Patients with Breast Cancer: A Systematic Review and Meta-Analysis of Prospective Studies.PLoS One. 2016 Feb 26;11(2):e0150285. doi: 10.1371/journal.pone.0150285. eCollection 2016. PLoS One. 2016. PMID: 26919589 Free PMC article.
References
-
- Passik SD, McDonald MV. Psychosocial aspects of upper extremity lymphedema in women treated for breast carcinoma. Cancer. 1998;83:2817–2820. - PubMed
-
- Tobin MB, Lacey HJ, Meyer L, Mortimer PS. The psychosocial morbidity of breast cancer-related arm swelling. Psychological morbidity of lymphedema. Cancer. 1993;72:3248–3252. - PubMed
-
- McMasters KM, Giuliano AE, Ross MI, Reintgen DS, Hunt KK, Byrd DR, Klimberg VS, Whitworth PW, Tafra LC, Edwards MJ. Sentinel-lymph-node biopsy for breast cancer--not yet the standard of care. N Engl J Med. 1998;339:990–995. 1998. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
