

Amygdalar atrophy in symptomatic Alzheimer's disease based on diffeomorphometry: the BIOCARD cohort
- PMID: 25444602
- PMCID: PMC4271320
- DOI: 10.1016/j.neurobiolaging.2014.06.032
Amygdalar atrophy in symptomatic Alzheimer's disease based on diffeomorphometry: the BIOCARD cohort
Abstract
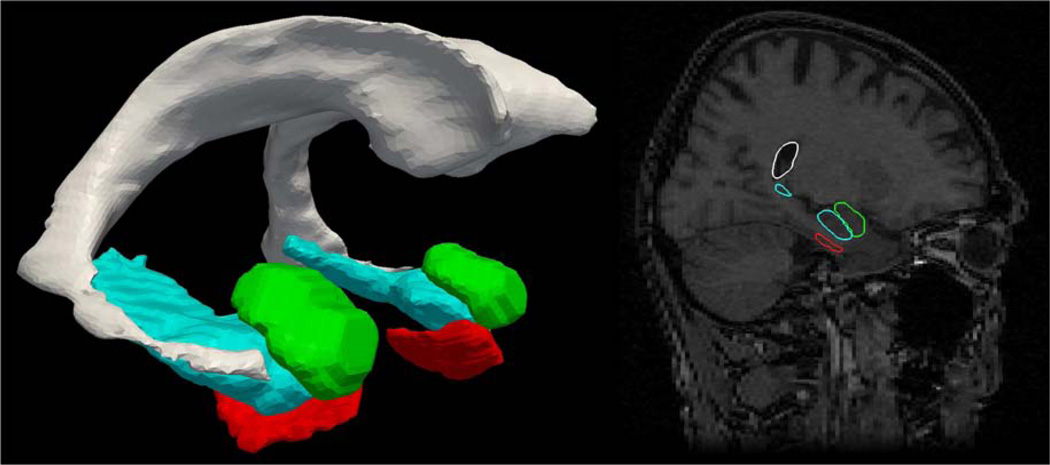
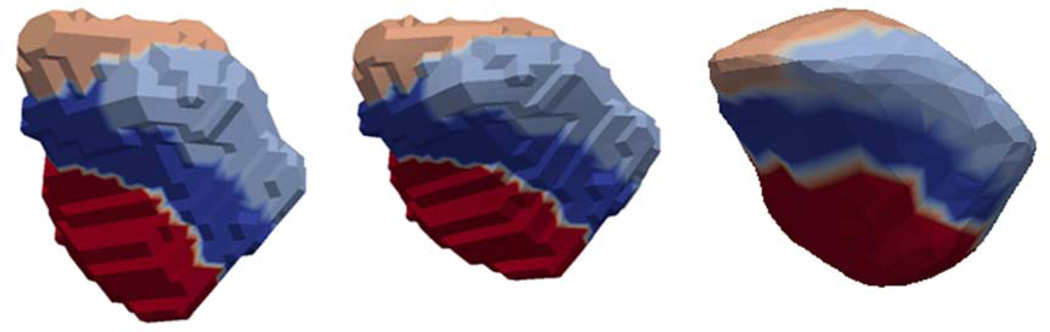
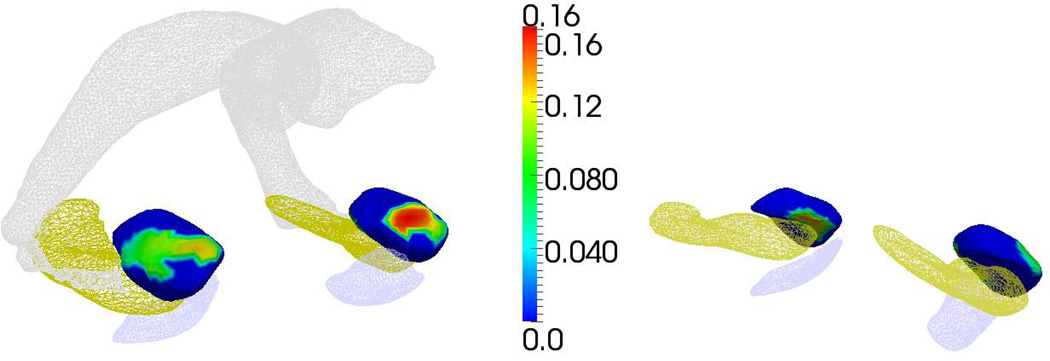
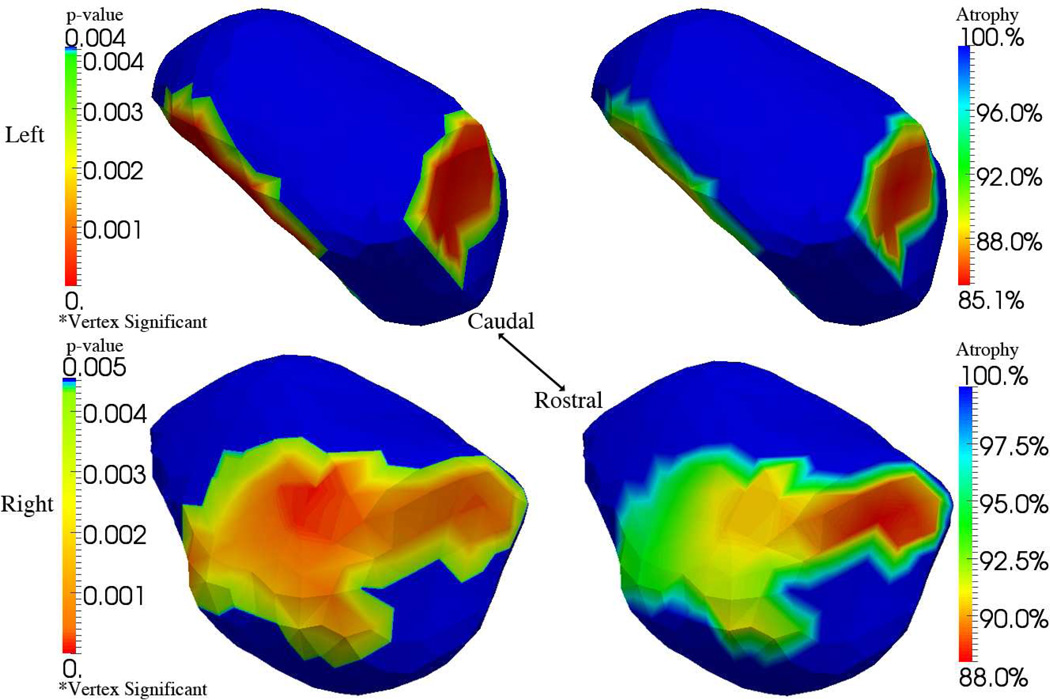
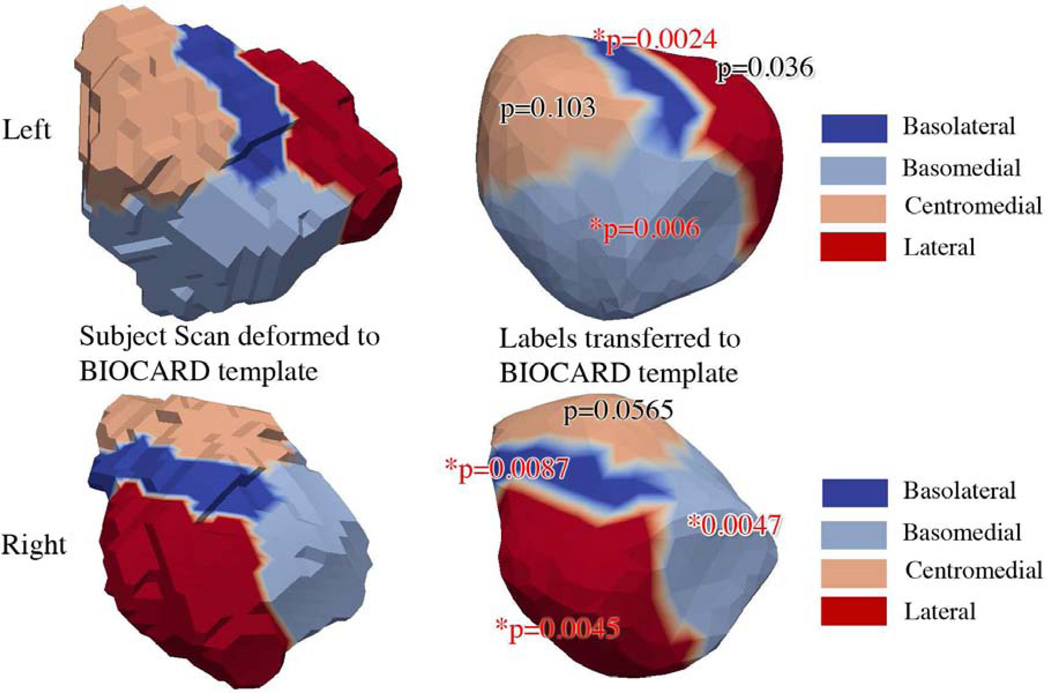
This article examines the diffeomorphometry of magnetic resonance imaging-derived structural markers for the amygdala, in subjects with symptomatic Alzheimer's disease (AD). Using linear mixed-effects models we show differences between those with symptomatic AD and controls. Based on template centered population analysis, the distribution of statistically significant change is seen in both the volume and shape of the amygdala in subjects with symptomatic AD compared with controls. We find that high-dimensional vertex based markers are statistically more significantly discriminating (p < 0.00001) than lower-dimensional markers and volumes, consistent with comparable findings in presymptomatic AD. Using a high-field 7T atlas, significant atrophy was found to be centered in the basomedial and basolateral subregions, with no evidence of centromedial involvement.
Keywords: Alzheimer's disease; Amygdala; MCI; MRI; Shape.
Copyright © 2015 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure Statement: All authors do not have conflicts of interest.
Figures
References
-
- Arnold SE, Hyman BT, Flory J, Damasio AR, Van Hoesen GW. The topographical and neuroanatomical distribution of neurofibrillary tangles and neuritic plaques in the cerebral cortex of patients with Alzheimer's disease. Cereb Cortex. 1991;1(1):103–116. - PubMed
-
- Arriagada PV, Growdon JH, Hedley-Whyte ET, Hyman BT. Neurofibrillary tangles but not senile plaques parallel duration and severity of Alzheimer's disease. Neurology. 1992;42(3 Pt 1):631–639. - PubMed
-
- Ashburner J, Csernansky JG, Davatzikos C, Fox NC, Frisoni GB, Thompson PM. Computer-assisted imaging to assess brain structure in healthy and diseased brains. Lancet Neurol. 2003;2(2):79–88. - PubMed
-
- Atiya M, Hyman BT, Albert MS, Killiany R. Structural magnetic resonance imaging in established and prodromal Alzheimer disease: a review. Alzheimer disease and associated disorders. 2003;17(3):177–195. - PubMed
-
- Beg MF, Miller MI, Trouve A, Younes L. Computing large deformation metric mappings via geodesic flows of diffeomorphisms. International Journal of Computer Vision. 2005;61(2):139–157.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
