

Clinical effectiveness and cost-effectiveness of quadrivalent human papillomavirus vaccination in HIV-negative men who have sex with men to prevent recurrent high-grade anal intraepithelial neoplasia
- PMID: 25444820
- PMCID: PMC4254641
- DOI: 10.1016/j.vaccine.2014.10.052
Clinical effectiveness and cost-effectiveness of quadrivalent human papillomavirus vaccination in HIV-negative men who have sex with men to prevent recurrent high-grade anal intraepithelial neoplasia
Abstract
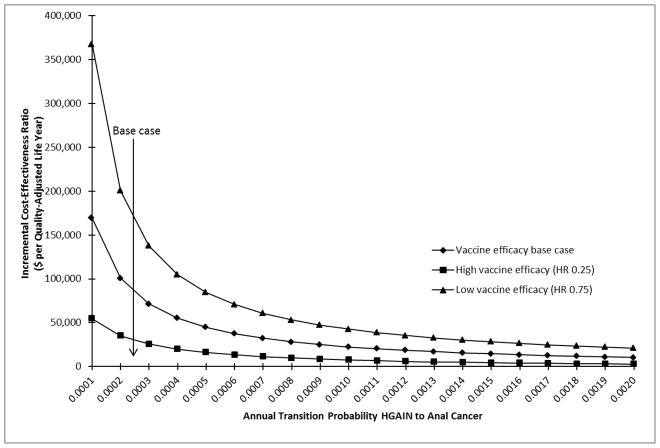
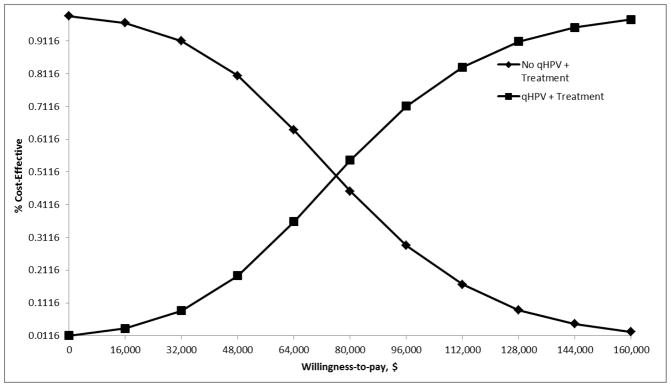
We examined the long-term clinical and economic benefits of quadrivalent human papillomavirus (qHPV) vaccine as a secondary/adjunct prevention strategy in the prevention of recurrent high-grade intraepithelial neoplasia (HGAIN) in HIV-negative men who have sex with men (MSM) and are 27 years or older. We constructed a Markov model to evaluate the clinical effectiveness and cost-effectiveness of two strategies: (1) no qHPV vaccine after treatment for HGAIN versus (2) qHPV vaccine after treatment for HGAIN. Model parameters, including natural history of anal cancer, vaccine efficacy measured in terms of hazard ratio (HR) (decrease in the risk of recurrent HGAIN), HGAIN treatment efficacy, utilities, and costs, were obtained from the literature. The outcomes were measured in terms of lifetime risk of anal cancer, lifetime cost, quality-adjusted life years, and incremental cost-effectiveness ratios (ICERs). Sensitivity analysis was conducted on all model parameters. We found that vaccinating HIV-negative MSM reduced the lifetime risk of anal cancer by 60.77% at an ICER of US$87,240 per quality-adjusted life-year. The results were highly sensitive to vaccine efficacy, transition of HGAIN to anal cancer, cost of treatment for HGAIN, vaccine degree of protection over time, and the vaccine duration of protection and less sensitive to HPV clearance, cost of qHPV vaccine, and the transitions from normal to low-grade anal intraepithelial neoplasia (LGAIN) and normal to HGAIN. With an HR of 0.3, the ICER was well below a $50,000 willingness-to-pay threshold; with an HR of 0.5, the ICER was still below a threshold of $100,000. The most critical disease-related factor influencing the cost-effectiveness was the progression of HGAIN to anal cancer. At an annual transition probability below 0.001, the ICER was below $50,000. Vaccinating HIV-negative MSM treated for HGAIN decreases the lifetime risk of anal cancer and is likely to be a cost-effective intervention.
Keywords: Anal neoplasia; Cost-effectiveness analysis; High-grade intraepithelial neoplasia; Human papillomavirus; Quadrivalent human papillomavirus vaccine; Secondary/adjunct prevention.
Published by Elsevier Ltd.
Conflict of interest statement
Figures

References
-
- Machalek DA, Poynten M, Jin F, Fairley CK, Farnsworth A, Garland SM, et al. Anal human papillomavirus infection and associated neoplastic lesions in men who have sex with men: a systematic review and meta-analysis. Lancet Oncol. 2012;13:487–500. - PubMed
-
- Gervaz P, Hahnloser D, Wolff BG, Anderson SA, Cunningham J, Beart RW, Jr, et al. Molecular biology of squamous cell carcinoma of the anus: a comparison of HIV-positive and HIV-negative patients. J Gastrointest Surg. 2004;8:1024–30. - PubMed
-
- Goldstone SE, Kawalek AZ, Huyett JW. Infrared coagulator: a useful tool for treating anal squamous intraepithelial lesions. Dis Colon Rectum. 2005;48:1042–54. - PubMed
-
- Goldstone RN, Goldstone AB, Russ J, Goldstone SE. Long-term follow-up of infrared coagulator ablation of anal high-grade dysplasia in men who have sex with men. Dis Colon Rectum. 2011;54:1284–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
