

The right ventricle in pulmonary arterial hypertension
- PMID: 25445946
- PMCID: PMC9487395
- DOI: 10.1183/09059180.00007414
The right ventricle in pulmonary arterial hypertension
Abstract
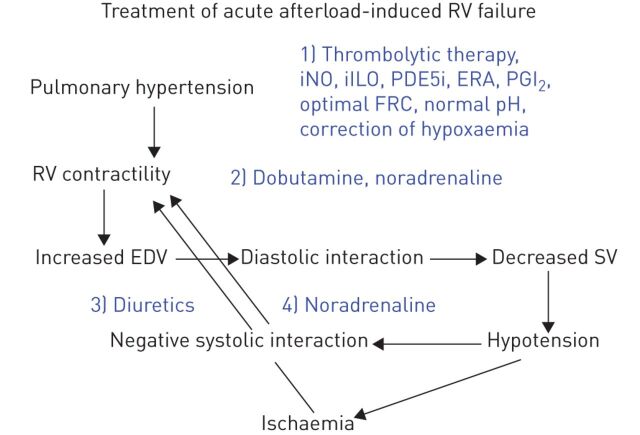
Pulmonary arterial hypertension (PAH) is a right heart failure syndrome. In early-stage PAH, the right ventricle tends to remain adapted to afterload with increased contractility and little or no increase in right heart chamber dimensions. However, less than optimal right ventricular (RV)-arterial coupling may already cause a decreased aerobic exercise capacity by limiting maximum cardiac output. In more advanced stages, RV systolic function cannot remain matched to afterload and dilatation of the right heart chamber progressively develops. In addition, diastolic dysfunction occurs due to myocardial fibrosis and sarcomeric stiffening. All these changes lead to limitation of RV flow output, increased right-sided filling pressures and under-filling of the left ventricle, with eventual decrease in systemic blood pressure and altered systolic ventricular interaction. These pathophysiological changes account for exertional dyspnoea and systemic venous congestion typical of PAH. Complete evaluation of RV failure requires echocardiographic or magnetic resonance imaging, and right heart catheterisation measurements. Treatment of RV failure in PAH relies on: decreasing afterload with drugs targeting pulmonary circulation; fluid management to optimise ventricular diastolic interactions; and inotropic interventions to reverse cardiogenic shock. To date, there has been no report of the efficacy of drug treatments that specifically target the right ventricle.
©ERS 2014.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside the online version of this article at
Figures
Similar articles
-
The right ventricle: interaction with the pulmonary circulation.Crit Care. 2016 Sep 10;20(1):266. doi: 10.1186/s13054-016-1440-0. Crit Care. 2016. PMID: 27613549 Free PMC article. Review.
-
Right Ventricular and Right Atrial Function Are Less Compromised in Pulmonary Hypertension Secondary to Heart Failure With Preserved Ejection Fraction: A Comparison With Pulmonary Arterial Hypertension With Similar Pressure Overload.Circ Heart Fail. 2022 Feb;15(2):e008726. doi: 10.1161/CIRCHEARTFAILURE.121.008726. Epub 2021 Dec 23. Circ Heart Fail. 2022. PMID: 34937392 Free PMC article.
-
Direct and indirect protection of right ventricular function by estrogen in an experimental model of pulmonary arterial hypertension.Am J Physiol Heart Circ Physiol. 2014 Aug 1;307(3):H273-83. doi: 10.1152/ajpheart.00758.2013. Epub 2014 Jun 6. Am J Physiol Heart Circ Physiol. 2014. PMID: 24906919 Free PMC article.
-
Pathophysiology of the right ventricle in health and disease: an update.Cardiovasc Res. 2023 Aug 19;119(10):1891-1904. doi: 10.1093/cvr/cvad108. Cardiovasc Res. 2023. PMID: 37463510
-
Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology.J Am Coll Cardiol. 2013 Dec 24;62(25 Suppl):D22-33. doi: 10.1016/j.jacc.2013.10.027. J Am Coll Cardiol. 2013. PMID: 24355638 Review.
Cited by
-
Changes in heart morphometric parameters over the course of a monocrotaline-induced pulmonary arterial hypertension rat model.J Transl Med. 2020 Jun 30;18(1):262. doi: 10.1186/s12967-020-02440-7. J Transl Med. 2020. PMID: 32605656 Free PMC article.
-
Echocardiographic estimation of right ventricular wall tension: haemodynamic comparison and long-term follow-up.Pulm Circ. 2019 Dec 27;9(4):2045894019895420. doi: 10.1177/2045894019895420. eCollection 2019 Oct-Dec. Pulm Circ. 2019. PMID: 31908767 Free PMC article.
-
Clinical Evaluation of Exercise Capacity in Adults with Systemic Right Ventricle.Tex Heart Inst J. 2019 Feb 1;46(1):14-20. doi: 10.14503/THIJ-17-6408. eCollection 2019 Feb. Tex Heart Inst J. 2019. PMID: 30833832 Free PMC article.
-
Organ-level right ventricular dysfunction with preserved Frank-Starling mechanism in a mouse model of pulmonary arterial hypertension.J Appl Physiol (1985). 2018 May 1;124(5):1244-1253. doi: 10.1152/japplphysiol.00725.2017. Epub 2018 Jan 25. J Appl Physiol (1985). 2018. PMID: 29369739 Free PMC article.
-
Computational quantification of patient-specific changes in ventricular dynamics associated with pulmonary hypertension.Am J Physiol Heart Circ Physiol. 2019 Dec 1;317(6):H1363-H1375. doi: 10.1152/ajpheart.00094.2019. Epub 2019 Nov 1. Am J Physiol Heart Circ Physiol. 2019. PMID: 31674809 Free PMC article.
References
-
- Hoeper MM, Bogaard HJ, Condliffe R, et al. . Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol 2013; 62: Suppl. 25, D45 D50 . - PubMed
-
- Vonk-Noordegraaf A, Haddad F, Chin KM, et al. . Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. J Am Coll Cardiol 2013; 62: Suppl. 25, D22 D33 . - PubMed
-
- Haddad F, Hunt SA, Rosenthal DN, et al. . Right ventricular function in cardiovascular disease, part I. Anatomy, physiology, aging and functional assessment of the right ventricle. Circulation 2008; 117: 1436–1448. - PubMed
-
- Guyton AC, Lindsey AW, Gilluly JJ. The limits of right ventricular compensation following acute increase in pulmonary circulatory resistance. Circ Res 1954; 2: 326–332. - PubMed
-
- Sagawa K, Maughan L, Suga H, eds, et al.. Cardiac Contraction and the Pressure-Volume Relationship. Oxford, Oxford University Press, 1988.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical