

Lung size mismatch and primary graft dysfunction after bilateral lung transplantation
- PMID: 25447586
- PMCID: PMC4329253
- DOI: 10.1016/j.healun.2014.09.030
Lung size mismatch and primary graft dysfunction after bilateral lung transplantation
Abstract
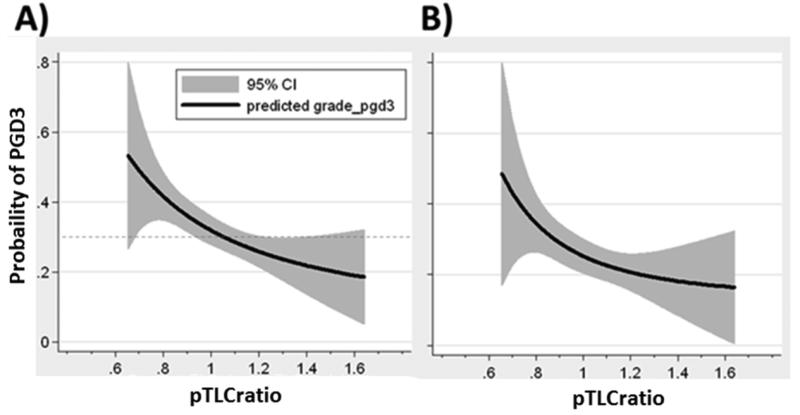
Background: Donor-to-recipient lung size matching at lung transplantation (LTx) can be estimated by the predicted total lung capacity (pTLC) ratio (donor pTLC/recipient pTLC). We aimed to determine whether the pTLC ratio is associated with the risk of primary graft dysfunction (PGD) after bilateral LTx (BLT).
Methods: We calculated the pTLC ratio for 812 adult BLTs from the Lung Transplant Outcomes Group between March 2002 to December 2010. Patients were stratified by pTLC ratio >1.0 ("oversized") and pTLC ratio ≤1.0 ("undersized"). PGD was defined as any ISHLT Grade 3 PGD (PGD3) within 72 hours of reperfusion. We analyzed the association between risk factors and PGD using multivariable conditional logistic regression. As transplant diagnoses can influence the size-matching decisions and also modulate the risk for PGD, we performed pre-specified analyses by assessing the impact of lung size mismatch within diagnostic categories.
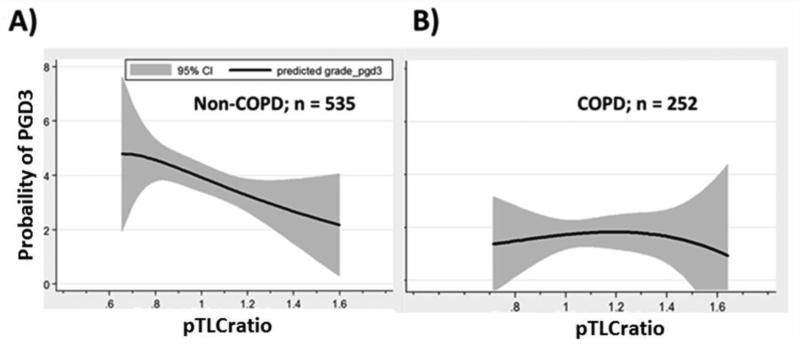
Results: In univariate analyses oversizing was associated with a 39% lower odds of PGD3 (OR 0.61, 95% CI, 0.45-0.85, p = 0.003). In a multivariate model accounting for center-effects and known PGD risks, oversizing remained independently associated with a decreased odds of PGD3 (OR 0.58, 95% CI 0.38 to 0.88, p = 0.01). The risk-adjusted point estimate was similar for the non-COPD diagnosis groups (OR 0.52, 95% CI 0.32 to 0.86, p = 0.01); however, there was no detected association within the COPD group (OR 0.72, 95% CI 0.29 to 1.78, p = 0.5).
Conclusion: Oversized allografts are associated with a decreased risk of PGD3 after BLT; this effect appears most apparent in non-COPD patients.
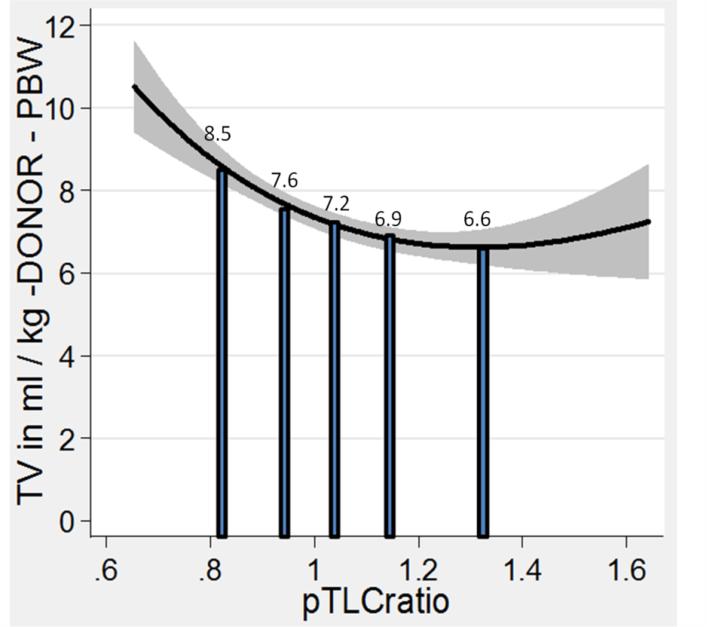
Keywords: lung size mismatch; lung transplantation; mechanical ventilation; primary graft dysfunction; tidal volume.
Copyright © 2015 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Eberlein M, Arnaoutakis GJ, Yarmus L, et al. The effect of lung size mismatch on complications and resource utilization after bilateral lung transplantation. J Heart Lung Transplant. 2012;31:492–500. - PubMed
-
- Eberlein M, Diehl E, Bolukbas S, et al. An oversized allograft is associated with improved survival after lung transplantation for idiopathic pulmonary arterial hypertension. J Heart Lung Transplant. 2013;32:1172–1178. - PubMed
-
- Eberlein M, Permutt S, Brown RH, et al. Supranormal expiratory airflow after bilateral lung transplantation is associated with improved survival. Am J Respir Crit Care Med. 2011;183:79–87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
