

Prognostic comparison of different sensitivity cardiac troponin assays in stable heart failure
- PMID: 25447612
- PMCID: PMC4340722
- DOI: 10.1016/j.amjmed.2014.09.029
Prognostic comparison of different sensitivity cardiac troponin assays in stable heart failure
Abstract
Background: Cardiac troponin (cTn) levels offer prognostic information for patients with heart failure. Highly sensitive assays detect levels of cTn much lower than the 99th percentile of standard cTn assays. We hypothesize that cardiac troponin levels measured by a high-sensitivity assay provide better prognostic value compared with cTn levels measured by a standard assay in patients with chronic heart failure.
Methods: We measured high-sensitivity cTnT (hs-cTnT) and standard cardiac troponin I (cTnI) levels, as well as amino-terminal pro B-type natriuretic peptide (NT-proBNP) in 504 sequential stable patients with a history of heart failure who underwent elective coronary angiography, without acute coronary syndrome, and with 5-year follow-up of all-cause mortality.
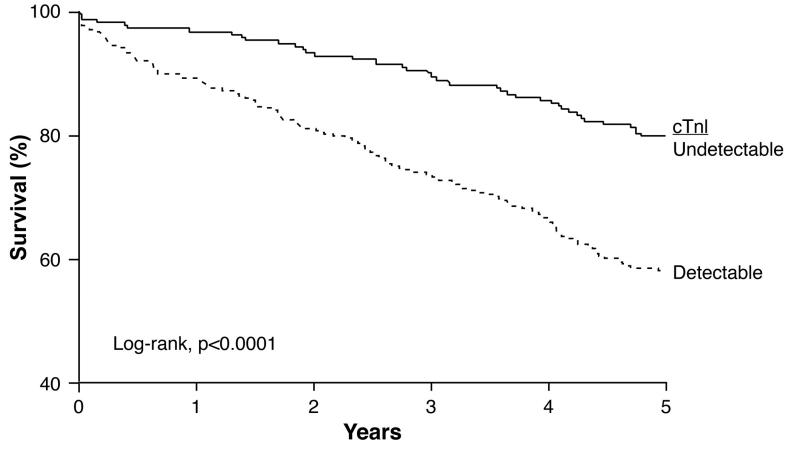
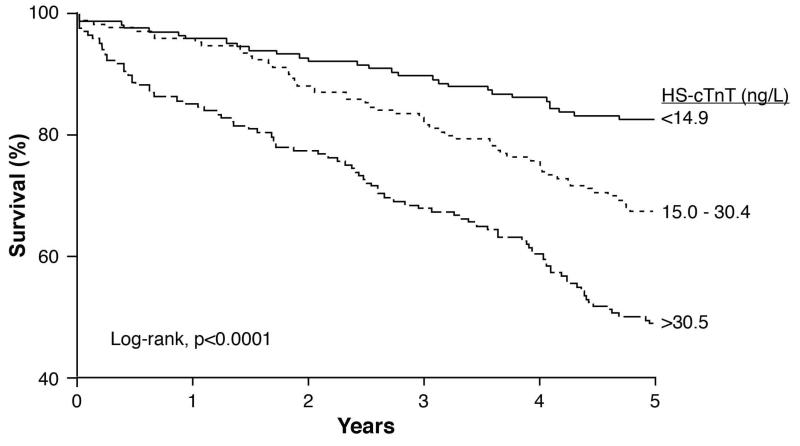
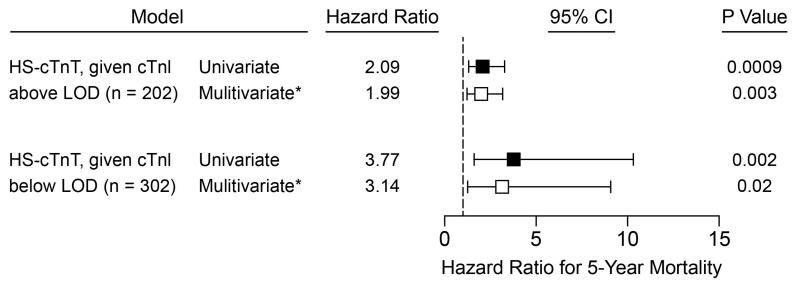
Results: The median hs-cTnT level was 21.2 (interquartile range 12.3-40.9) ng/L and 170 subjects died over 5 years. In a head-to-head overall comparison, hs-cTnT provided increased prognostic utility compared with cTnI (area under the curve [AUC] 66.1% and AUC 69.4%, respectively, P = .03; 9.0% integrated discrimination improvement, P < .001; and 13.6% event-specific reclassification, P < .001), and was independent of NT-proBNP and renal function. Even within the subset of patients where cTn levels by both assays were above the limit of quantification, higher hs-cTnT is associated with a 2-fold increase in 5-year mortality risk after adjusting for traditional risk factors (tertile 1 vs 3: hazard ratio [95% confidence interval] 2.0 [1.3-3.2]; P = .0002).
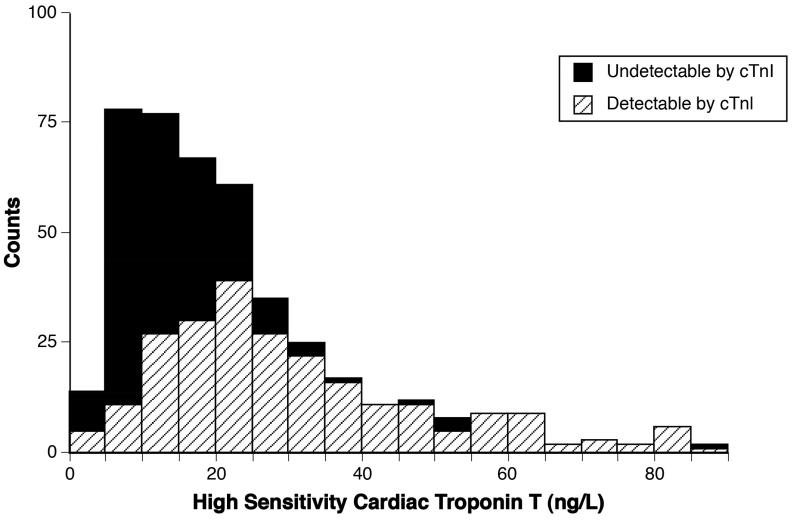
Conclusion: Cardiac troponin can be detected by the high-sensitivity assay in more patients with chronic heart failure than the standard assay, and may yield independent and better prognostic accuracy for mortality prediction than standard assay.
Keywords: Cardiac troponin; Heart failure; High-sensitivity cardiac troponin; Prognosis.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50(22):2173–95. - PubMed
-
- Peacock WFt, De Marco T, Fonarow GC, et al. Cardiac troponin and outcome in acute heart failure. N Engl J Med. 2008;358(20):2117–26. - PubMed
-
- Kociol RD, Pang PS, Gheorghiade M, et al. Troponin elevation in heart failure prevalence, mechanisms, and clinical implications. J Am Coll Cardiol. 2010;56(14):1071–8. - PubMed
-
- Wu AH. Increased troponin in patients with sepsis and septic shock: myocardial necrosis or reversible myocardial depression? Intensive Care Med. 2001;27(6):959–61. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
