

Ten-year incident osteoporosis-related fractures in the population-based Canadian Multicentre Osteoporosis Study - comparing site and age-specific risks in women and men
- PMID: 25451323
- PMCID: PMC5092162
- DOI: 10.1016/j.bone.2014.10.026
Ten-year incident osteoporosis-related fractures in the population-based Canadian Multicentre Osteoporosis Study - comparing site and age-specific risks in women and men
Abstract
Background: Population-based incident fracture data aid fracture prevention and therapy decisions. Our purpose was to describe 10-year site-specific cumulative fracture incidence by sex, age at baseline, and degree of trauma with/without consideration of competing mortality in the Canadian Multicentre Osteoporosis Study adult cohort.
Methods: Incident fractures and mortality were identified by annual postal questionnaires to the participant or proxy respondent. Date, site and circumstance of fracture were gathered from structured interviews and medical records. Fracture analyses were stratified by sex and age at baseline and used both Kaplan-Meier and competing mortality methods.
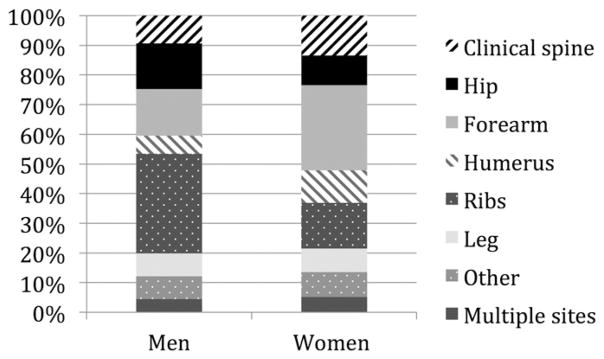
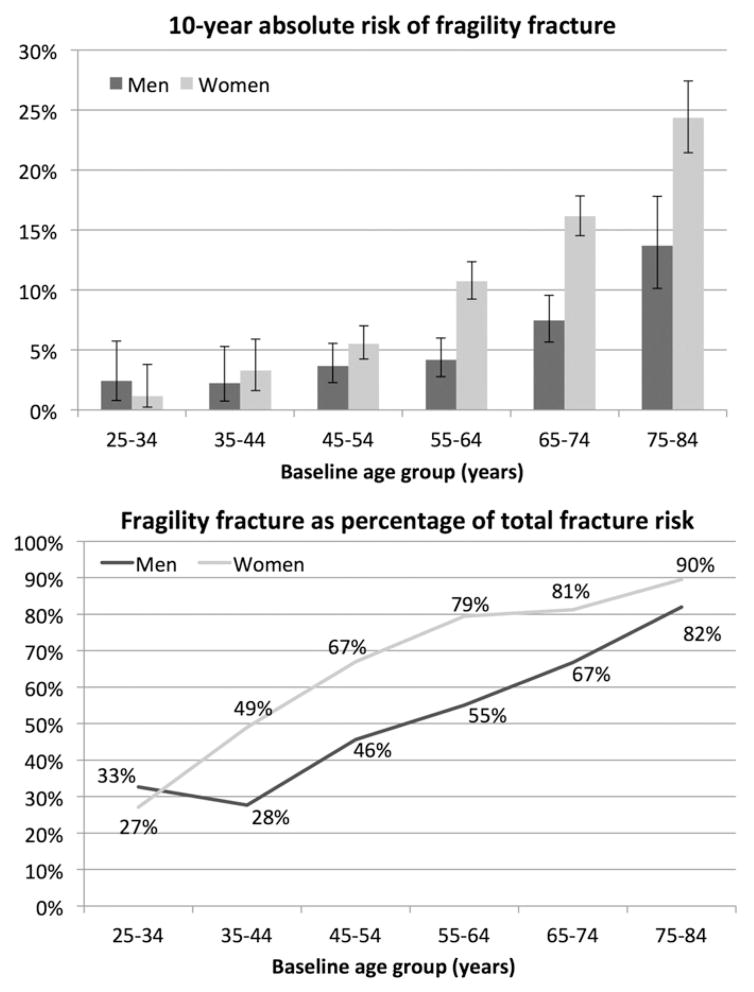
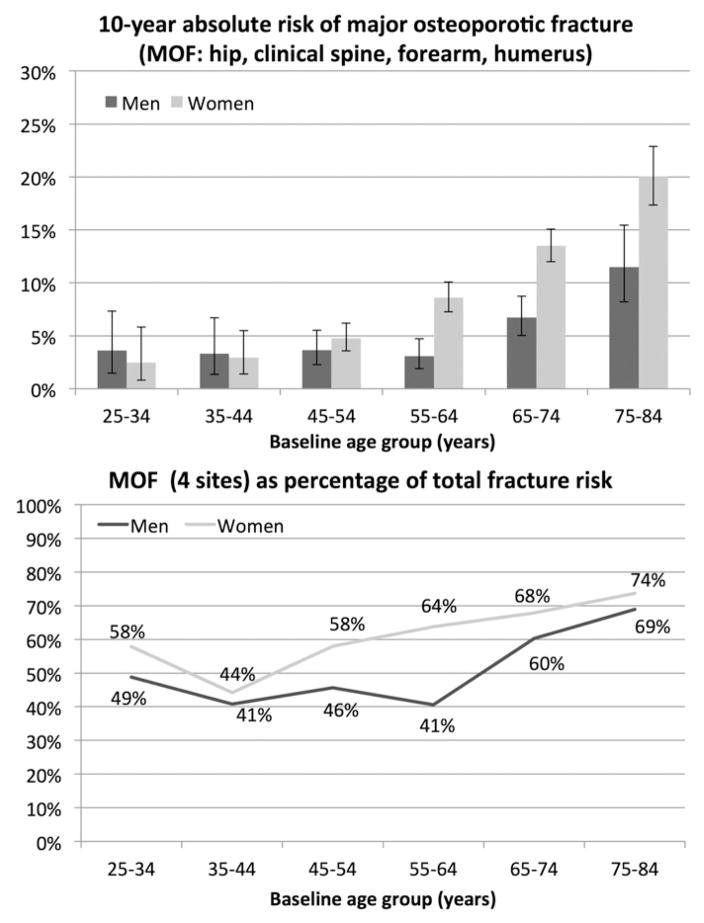
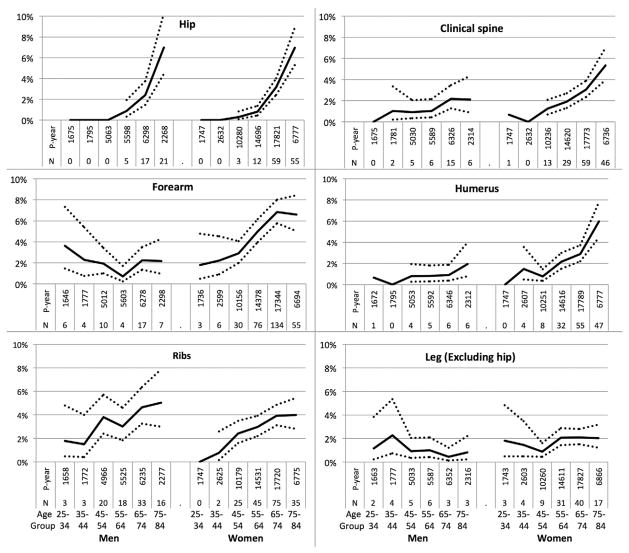
Results: The baseline (1995-97) cohort included 6314 women and 2789 men (aged 25-84 years; mean±SD 62±12 and 59±14, respectively), with 4322 (68%) women and 1732 (62%) men followed to year-10. At least one incident fracture occurred for 930 women (14%) and 247 men (9%). Competing mortality exceeded fracture risk for men aged 65+years at baseline. Age was a strong predictor of incident fractures especially fragility fractures, with higher age gradients for women vs. men. Major osteoporotic fracture (MOF) (hip, clinical spine, forearm, humerus) accounted for 41-74% of fracture risk by sex/age strata; in women all MOF sites showed age-related increases but in men only hip was clearly age-related. The most common fractures were the forearm for women and the ribs for men. Hip fracture incidence was the highest for the 75-84 year baseline age-group with no significant difference between women 7.0% (95% CI 5.3, 8.9) and men 7.0% (95% CI 4.4, 10.3).
Interpretation: There are sex differences in the predominant sites and age-gradients of fracture. In older men, competing mortality exceeds cumulative fracture risk.
Keywords: 10-year fracture incidence; Clinical vertebral fracture; Fracture prediction; Hip fracture; Population-based; Sex.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
References
-
- Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res. 2007;22:465–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
