

Risk of breast cancer in symptomatic women in primary care: a case-control study using electronic records
- PMID: 25452544
- PMCID: PMC4240152
- DOI: 10.3399/bjgp14X682873
Risk of breast cancer in symptomatic women in primary care: a case-control study using electronic records
Abstract
Background: Breast cancer is the most common cancer in the UK. GPs are encouraged to refer all women whose symptoms may represent cancer, rather than selecting those at highest risk.
Aim: To identify and quantify features of breast cancer in primary care.
Design and setting: A UK case-control study using the Clinical Practice Research Database (CPRD).
Method: Possible features of breast cancer were identified in the year before diagnosis, and odds ratios calculated using conditional logistic regression. Positive predictive values (PPVs) were estimated for consulting women.
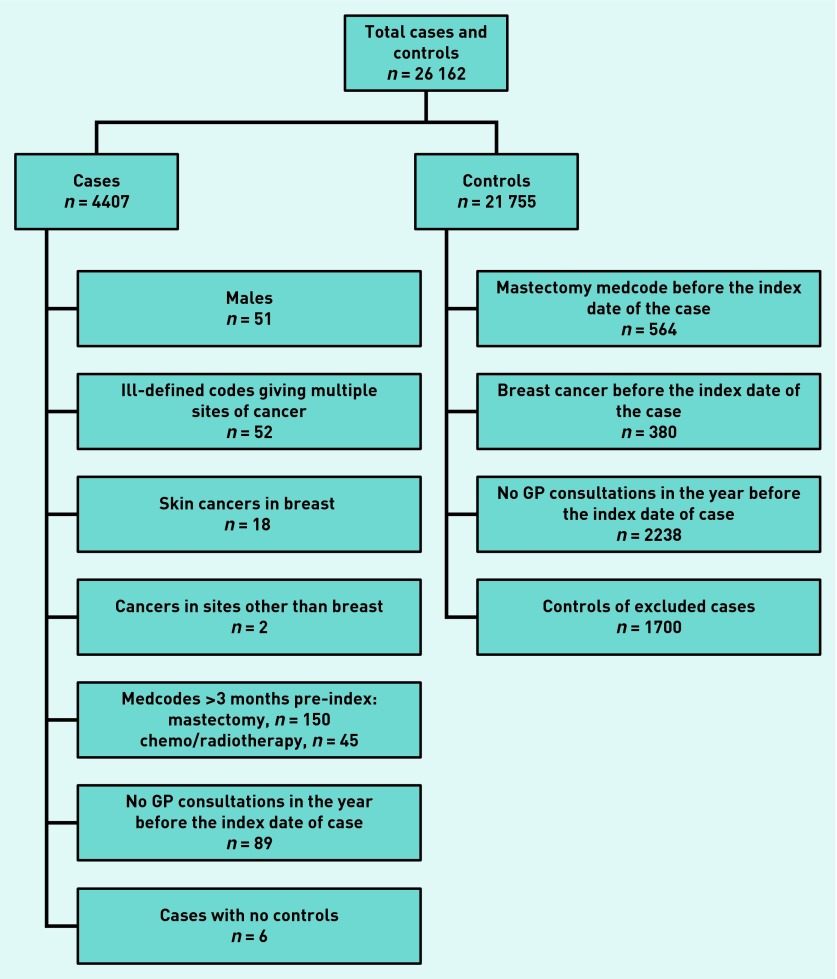
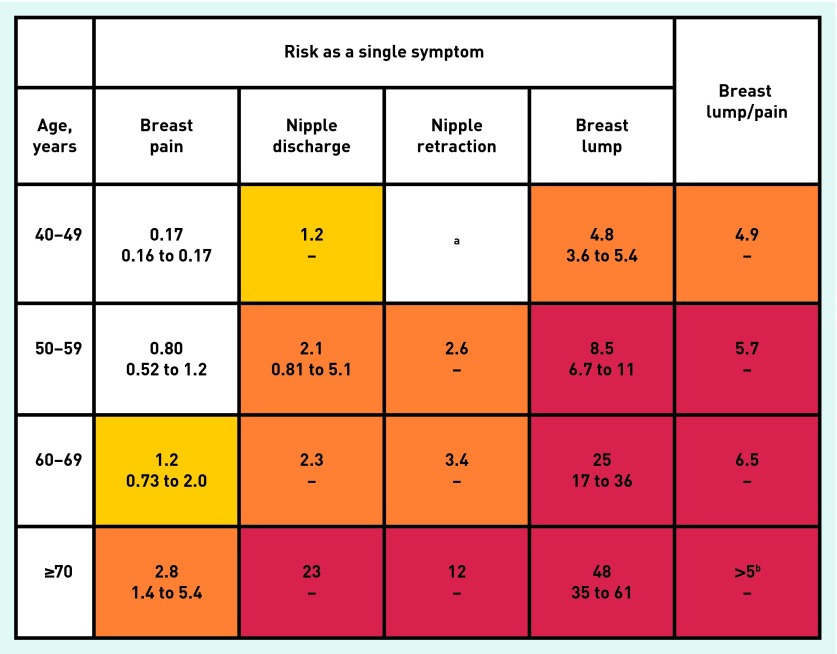
Results: A total of 3994 women aged ≥40 years with breast cancer between 2000 and 2009, and 16 873 age-, sex-, and practice-matched controls were studied. Median age at diagnosis was 63 years (interquartile range 55-74 years). Four features were significantly associated with breast cancer: breast lump (odds ratio [OR] 110; 95% confidence interval [CI] = I88 to 150), breast pain (OR = 4.2; 95% CI = 3.0 to 6.0), nipple retraction (OR = 26; 95% CI = 10 to 64), nipple discharge (OR = 19; 95% CI = 8.6 to 41): all P-values <0.01. In the year before diagnosis, 1762 (44%) of cases had a breast lump compared with 132 (0.8%) controls. The PPV of breast cancer with a breast lump was 4.8% in women aged 40-49 years, rising to 48% in women aged >70 years. PPVs were lower in women who also reported breast pain.
Conclusion: Generally, the figures support current referral practice. However, the low likelihood of cancer for all the non-lump symptoms means that the current guidance recommends investigation for possible cancer at a more liberal risk threshold than for other cancers. Although supported by patients, this may not meet current NHS criteria for cost-benefit.
Keywords: breast cancer; diagnosis; primary health care.
© British Journal of General Practice 2014.
Figures
References
-
- Cancer Research UK. CancerStats — incidence 2009 — UK. London: Cancer Research UK; 2012. http://publications.cancerresearchuk.org/downloads/Product/CS_CS_INCIDEN... (accessed 14 Oct 2014)
-
- Health and Social Care Information Centre. Breast screening programme, England, 2011–12. Leeds: HSCIC; 2013. https://catalogue.ic.nhs.uk/publications/screening/breast/bres-scre-prog... (accessed 14 Oct 2014)
-
- Willett A, Michell MJ, Lee MJR. Best practice diagnostic guidelines for patients presenting with breast symptoms. COI; 2010. http://www.associationofbreastsurgery.org.uk/media/4585/best_practice_di... (accessed 14 Oct 2014)
-
- National Institute for Health and Care Excellence. Referral guidelines for suspected cancer. London: NICE; 2005. NICE clinical guideline 27 (CG27) https://www.nice.org.uk/guidance/cg27/resources/guidance-referral-guidel... (accessed 14 Oct 2014)
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical