

Whole-genome sequencing and epidemiological analysis do not provide evidence for cross-transmission of mycobacterium abscessus in a cohort of pediatric cystic fibrosis patients
- PMID: 25452595
- PMCID: PMC4357290
- DOI: 10.1093/cid/ciu967
Whole-genome sequencing and epidemiological analysis do not provide evidence for cross-transmission of mycobacterium abscessus in a cohort of pediatric cystic fibrosis patients
Abstract
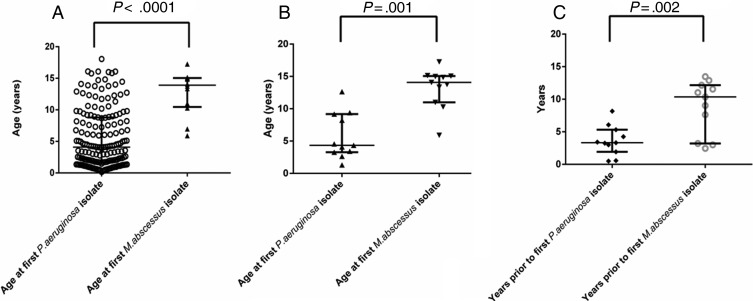
Background: Mycobacterium abscessus has emerged as a major pathogen in cystic fibrosis (CF) patients and has been associated with poor clinical outcomes, particularly following lung transplant. We investigated the acquisition of this bacterium in a cohort of pediatric CF patients.
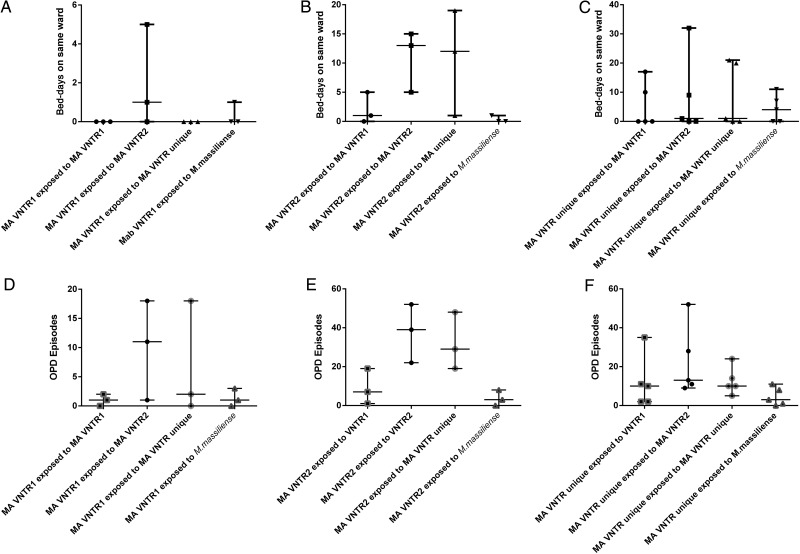
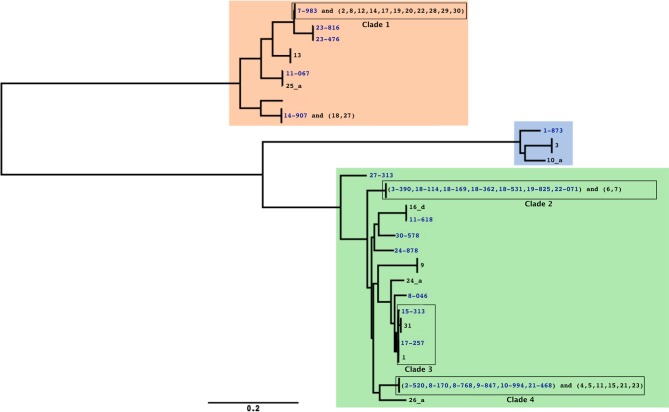
Methods: Demographic and patient location data were used to uncover epidemiological links between patients with genetically related strains of M. abscessus that had been previously typed by variable-number tandem repeat profiling. Whole-genome sequencing was applied to 27 M. abscessus isolates from the 20 patients in this cohort to provide definitive data on the genetic relatedness of strains.
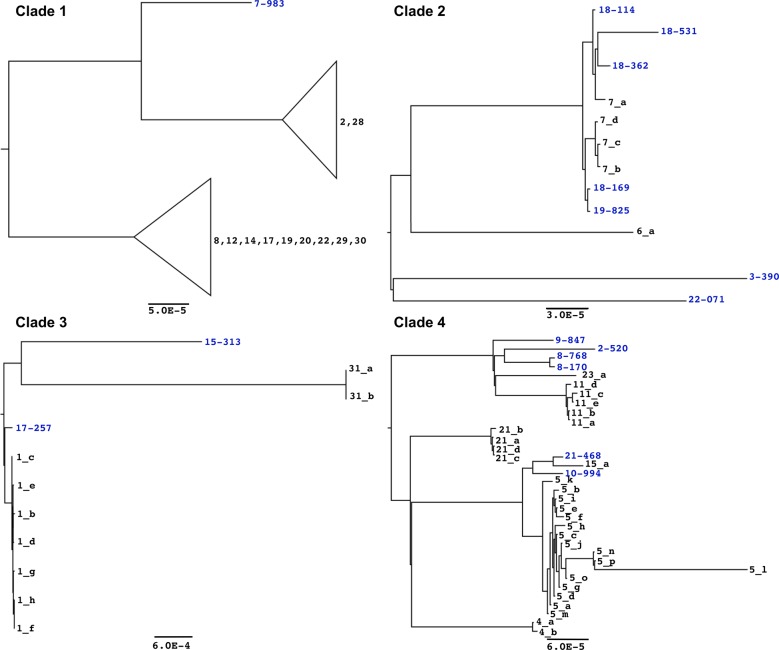
Results: Whole-genome sequencing data demonstrated that M. abscessus isolates from 16 patients were unrelated, differing by at least 34 single-nucleotide polymorphisms (SNPs) from any other isolate, suggesting that independent acquisition events have occurred. Only 2 clusters of very closely related (<25 SNPs) isolates from different patients were seen. The first cluster contained 8 isolates, differing by a maximum of 17 SNPs, from a sibling pair who had intense exposure to each other both inside and outside the hospital. The second cluster contained 3 isolates, differing by a maximum of 24 SNPs, from 2 individuals with no apparent epidemiological links.
Conclusions: We have not demonstrated cross-transmission of M. abscessus within our hospital, except between 1 sibling pair. Alternative routes of acquisition of M. abscessus infection, in particular the environment, require further investigation.
Keywords: Mycobacterium abscessus; VNTR; cross-transmission; cystic fibrosis; whole-genome sequencing.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Figures
References
-
- Gilljam M, Schersten H, Silverborn M, Jonsson B, Ericsson Hollsing A. Lung transplantation in patients with cystic fibrosis and Mycobacterium abscessus infection. J Cyst Fibros. 2010;9:272–6. - PubMed
-
- Luong ML, Morrissey O, Husain S. Assessment of infection risks prior to lung transplantation. Curr Opin Infect Dis. 2010;23:578–83. - PubMed
-
- Watkins RR, Lemonovich TL. Evaluation of infections in the lung transplant patient. Curr Opin Infect Dis. 2012;25:193–8. - PubMed
-
- Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175:367–416. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
