

Review
doi: 10.1542/pir.35-12-519.
Respiratory syncytial virus infection and bronchiolitis
Affiliations
- PMID: 25452661
- PMCID: PMC5029757
- DOI: 10.1542/pir.35-12-519
Item in Clipboard
Review
Respiratory syncytial virus infection and bronchiolitis
Pediatr Rev.
2014 Dec.
Erratum in
-
Correction.Pediatr Rev. 2015 Feb;36(2):85. doi: 10.1542/pir.36-2-85. Pediatr Rev. 2015. PMID: 25646315 Free PMC article. No abstract available.
No abstract available
Figures
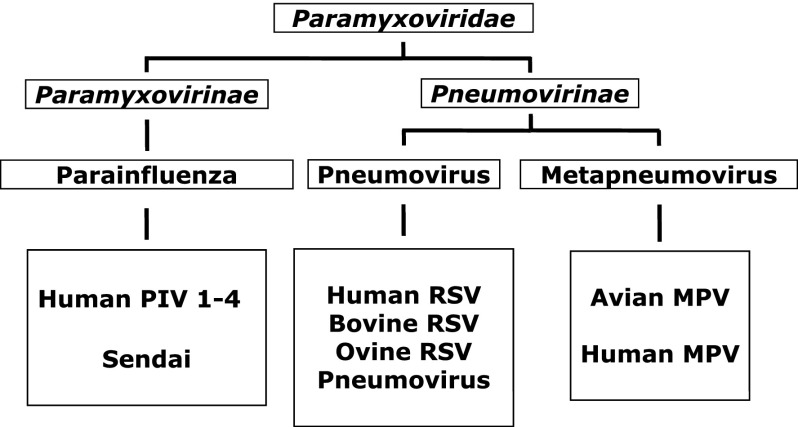
Respiratory syncytial virus (RSV) classification. Human RSV is an enveloped,
nonsegmented, negative-strand RNA virus of the Paramyxoviridae family, genus
Pneumovirus. The closely related
Metapneumovirus genus was considered an exclusively avian
virus until the discovery of a human strain in 2001.
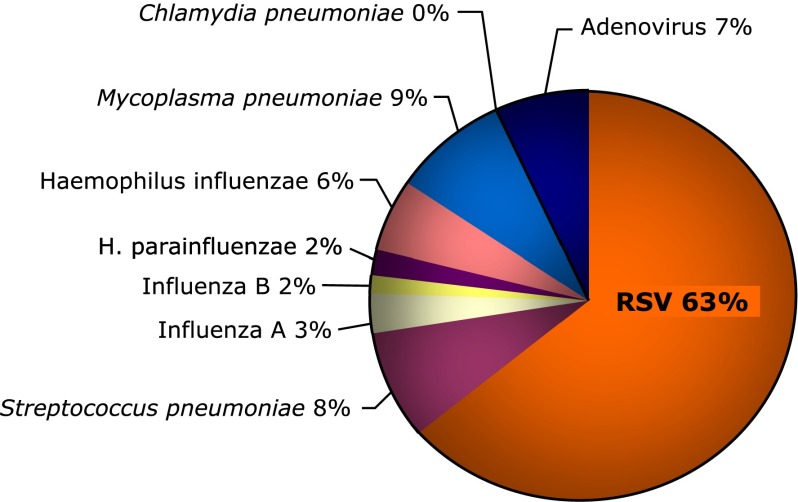
Etiology of acute respiratory infections in children. The World Health
Organization estimates indicate that respiratory syncytial virus (RSV) accounts
worldwide for more than 60% of acute respiratory infections in children and more
than 80% in infants younger than 1 year and at the peak of viral season.
Therefore, RSV is by far the most frequent cause of pediatric bronchiolitis and
pneumonia.
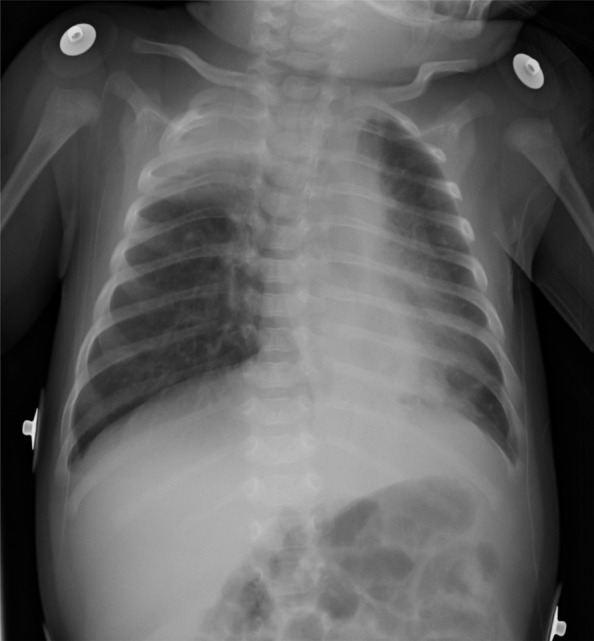
Clinical manifestations of respiratory syncytial virus (RSV). Chest radiography
performed in a child with RSV bronchiolitis revealed bilateral hyperinflation from
air trapping, patchy atelectasis from airway plugging, and peribronchial
thickening from lymphomonocytic infiltration. Patients with severe disease may
also have features more consistent with pneumonia, with areas of interstitial
parenchymal infiltration.
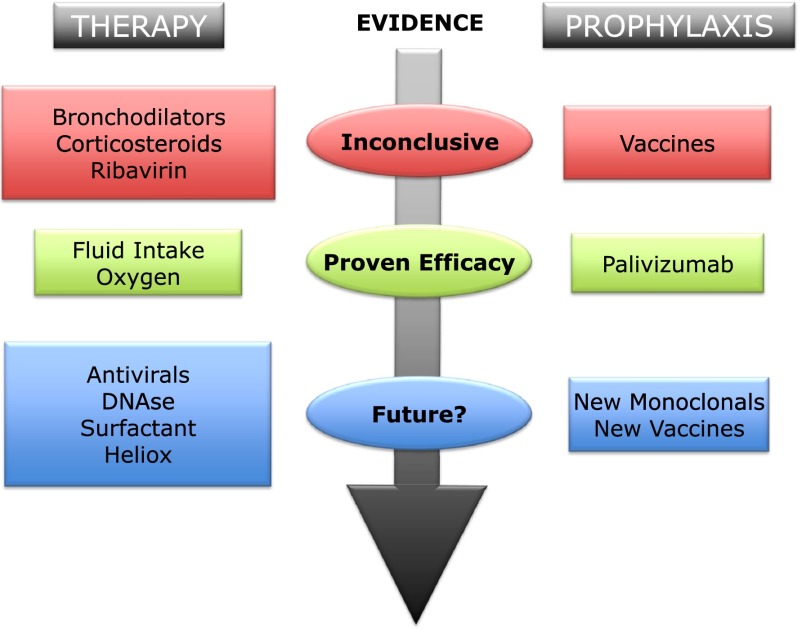
Evidence-based management of bronchiolitis. Passive prophylaxis is a safe and
effective way of protecting infants at risk for severe respiratory syncytial
virus (RSV) disease but is not cost-efficient. Once the infection is
established, the mainstay of current therapy remains supportive care because no
solid scientific evidence supporting the use of any conventional or
experimental pharmacologic agent currently exists. For the future, promising
antiviral molecules and new-generation humanized monoclonal antibodies are
being investigated, and structural biology may overcome the challenges that
have so far prevented the development of a safe and effective RSV vaccine.
References
-
- Ralston S, et al. Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis. Pediatrics. 2014;134(5):e1474–e1502. Accessed October 28, 2014, at: http://pediatrics.aappublications.org/content/134/5/e1474.full - PubMed
-
- Hall CB, Douglas RG., Jr Modes of transmission of respiratory syncytial virus. J Pediatr. 1981;99(1):100–103 - PubMed
-
- Gadomski AM, Bhasale AL. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev. 2006;3(3):CD001266. - PubMed
-
- Patel H, Platt R, Lozano JM, Wang EE. Glucocorticoids for acute viral bronchiolitis in infants and young children. Cochrane Database Syst Rev. 2004; (3):CD004878. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
