

The assisted bidirectional Glenn: a novel surgical approach for first-stage single-ventricle heart palliation
- PMID: 25454920
- PMCID: PMC6089632
- DOI: 10.1016/j.jtcvs.2014.10.035
The assisted bidirectional Glenn: a novel surgical approach for first-stage single-ventricle heart palliation
Abstract
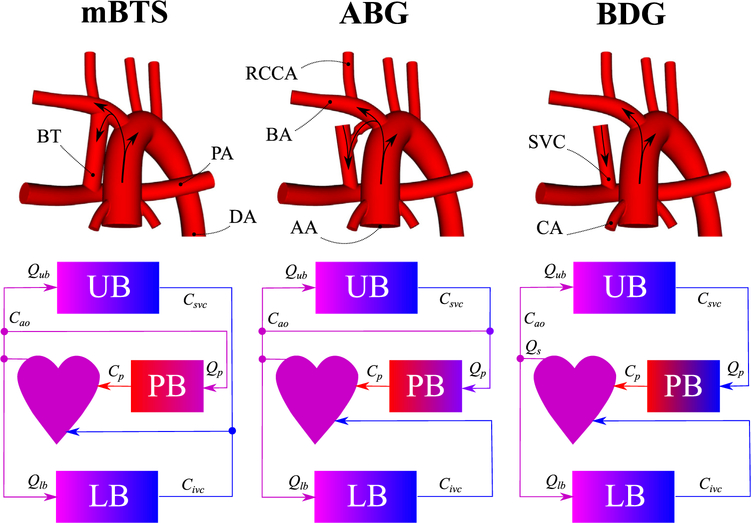
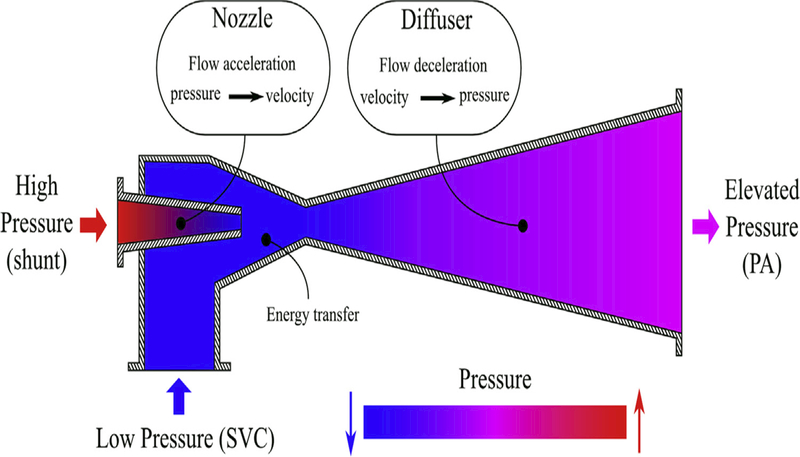
Background: Outcomes after a modified Blalock-Taussig shunt (mBTS) in neonates with single-ventricle physiology remain unsatisfactory. However, initial palliation with a superior cavopulmonary connection, such as a bidirectional Glenn (BDG), is discouraged, owing to potential for inadequate pulmonary blood flow (PBF). We tested the feasibility of a novel surgical approach, adopting the engineering concept of an ejector pump, whereby the flow in the BDG is "assisted" by injection of a high-energy flow stream from the systemic circulation.
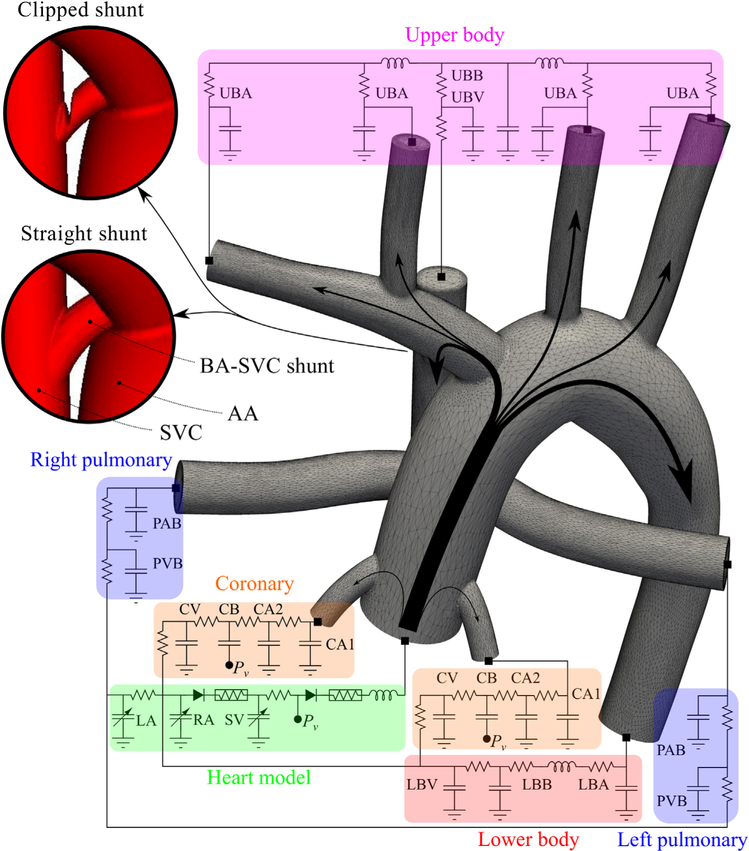
Methods: Realistic 3-dimensional models of the neonatal mBTS and BDG circulations were created. The "assisted" bidirectional Glenn (ABG) consisted of a shunt between the right innominate artery and the superior vena cava (SVC), with a 1.5-mm clip near the SVC anastomosis to create a Venturi effect. The 3 models were coupled to a validated hydraulic circulation model, and 2 pulmonary vascular resistance (PVR) values (7 and 2.3 Wood units) were simulated.
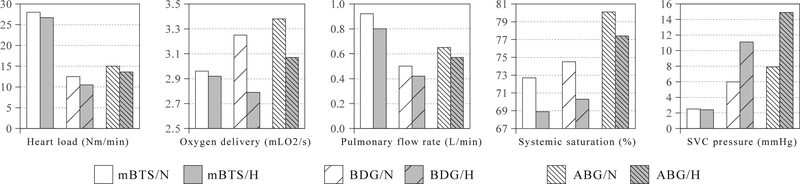
Results: The ABG provided the highest systemic oxygen saturation and oxygen delivery at both PVR levels. In addition to achieving higher PBF than the BDG, the ABG produced a lower single-ventricular workload than mBTS. SVC pressure was highest in the ABG model (ABG: 15; Glenn: 11; mBTS: 3 mm Hg; PVR = 7 Wood units), but at low PVR, the SVC pressure was significantly lower (ABG: 8; Glenn: 6; mBTS: <3 mm Hg).
Conclusions: Adopting the principle of an ejector pump, with additional flow directed into the SVC in a BDG, the ABG appears to increase PBF with a modest increase in SVC and pulmonary arterial pressure. Although multiscale modeling results demonstrate the conceptual feasibility of the ABG circulation, further technical refinement and investigations are necessary, especially in an appropriate animal model.
Copyright © 2015 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The steam locomotive makes a comeback: a new solution to staged single-ventricle palliation?J Thorac Cardiovasc Surg. 2015 Mar;149(3):706-7. doi: 10.1016/j.jtcvs.2014.11.064. Epub 2014 Nov 27. J Thorac Cardiovasc Surg. 2015. PMID: 25630859 No abstract available.
References
-
- Norwood W, Kirklin J, Sanders S. Hypoplastic left heart syndrome: experience with palliative surgery. Am J Cardiol. 1980;45:87–91. - PubMed
-
- Norwood W, Lang P, Castaneda A, Campbell D. Experience with operations for hypoplastic left heart syndrome. J Thorac Cardiovasc Surg. 1981;82:511–9. - PubMed
-
- Wong R, Baum V, Sangwan S. Truncus arteriosus: recognition and therapy of intra-operative cardiac ischemia. Anesthesiology. 1991;74:378–80. - PubMed
-
- Bartram U, Grnenfelder J, Praagh RV. Causes of death after the modified Norwood procedure: a study of 122 postmortem cases. Ann Thorac Surg. 1997;64:1795–802. - PubMed
-
- Tamisier D, Vouhe P, Vernant F, Leca F, Massot C, Neveux J. Modified Blalock-Taussig shunts: results in infants less than 3 months of age. Ann Thorac Surg. 1990;49:797–801. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
