

Prevalence of radiographic findings in individuals with chronic low back pain screened for a randomized controlled trial: secondary analysis and clinical implications
- PMID: 25455834
- PMCID: PMC4274221
- DOI: 10.1016/j.jmpt.2014.10.003
Prevalence of radiographic findings in individuals with chronic low back pain screened for a randomized controlled trial: secondary analysis and clinical implications
Abstract
Objective: The purpose of this study is to measure the prevalence of graded disc degeneration, spondylolisthesis, transitional segmentation, and the distribution of sacral slope in patients 21 to 65 years of age with chronic low back pain (CLBP).
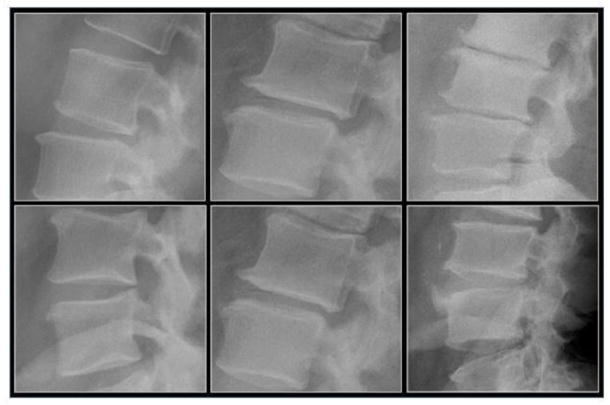
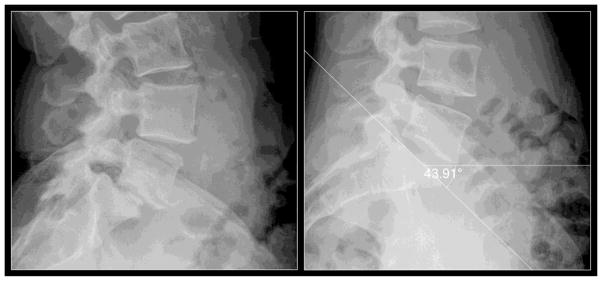
Methods: This retrospective study analyzed 247 digital lumbar radiographic series obtained during a randomized controlled trial of chiropractic patients with CLBP. Chronic low back pain was defined as pain in the low back lasting 12 weeks or longer. Radiographic findings of disc degeneration, spondylolisthesis, and lumbosacral transitional segmentation were graded by 2 authors using established classification criteria. Sacral slope was measured with a digital tool contained within imaging software.
Results: Lumbosacral transitional segments graded I to IV (Castellvi classification) were present in 14% of cases. Lumbar disc degeneration was most prevalent at L3-4 (49%), followed by L4-5 (42%), L2-3 (41%), L5-S1 (37%), and L1-2 (29%). Isthmic spondylolisthesis was present in 5% of cases, with L5 the most common location. Degenerative spondylolisthesis demonstrated a prevalence of 18%, most commonly occurring at L4. The prevalence of degenerative spondylolisthesis was 51% for women aged 50 to 59 years and 24% for men in the same age range.
Conclusions: Moderate-severe disc degeneration, multilevel disc narrowing, and degenerative spondylolisthesis were common in individuals with CLBP with age more than 40 years. Isthmic spondylolisthesis was not more prevalent than what has been reported in other populations. Transitional segmentation was identified in a minority of participants, with some of these exhibiting accessory joints or fusion. Mean sacral slope in individuals with CLBP was not substantially different from mean slopes reported in other populations.
Keywords: Chiropractic; Intervertebral Disc Degeneration; Low Back Pain; Lumbosacral Region; Prevalence; Radiography; Spondylolisthesis.
Copyright © 2014 National University of Health Sciences. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
CONFLICTS OF INTEREST
No conflicts of interest were reported for this study.
Figures

References
-
- Chou R, Fu R, Carrino JA, Deyo RA. Imaging strategies for low-back pain: systematic review and meta-analysis. Lancet. 2009 Feb 7;373(9662):463–72. - PubMed
-
- Ammendolia C, Bombardier C, Hogg-Johnson S, Glazier R. Views on radiography use for patients with acute low back pain among chiropractors in an Ontario community. J Manipulative Physiol Ther. 2002 Oct;25(8):511–20. - PubMed
-
- Chou R, Qaseem A, Snow V, Casey D, Cross JT, Jr, Shekelle P, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007 Oct 2;147(7):478–91. - PubMed
-
- Bussieres AE, Taylor JA, Peterson C. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults-an evidence-based approach-part 3: spinal disorders. J Manipulative Physiol Ther. 2008 Jan;31(1):33–88. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
