

Assessment of empirical antibiotic therapy optimisation in six hospitals: an observational cohort study
- PMID: 25455989
- PMCID: PMC5525058
- DOI: 10.1016/S1473-3099(14)70952-1
Assessment of empirical antibiotic therapy optimisation in six hospitals: an observational cohort study
Abstract
Background: Modification of empirical antimicrobials when warranted by culture results or clinical signs is recommended to control antimicrobial overuse and resistance. We aimed to assess the frequency with which patients were started on empirical antimicrobials, characteristics of the empirical regimen and the clinical characteristics of patients at the time of starting antimicrobials, patterns of changes to empirical therapy at different timepoints, and modifiable factors associated with changes to the initial empirical regimen in the first 5 days of therapy.
Methods: We did a chart review of adult inpatients receiving one or more antimicrobials in six US hospitals on 4 days during 2009 and 2010. Our primary outcome was the modification of antimicrobial regimen on or before the 5th day of empirical therapy, analysed as a three-category variable. Bivariate analyses were used to establish demographic and clinical variables associated with the outcome. Variables with p values below 0·1 were included in a multivariable generalised linear latent and mixed model with multinomial logit link to adjust for clustering within hospitals and accommodate a non-binary outcome variable.
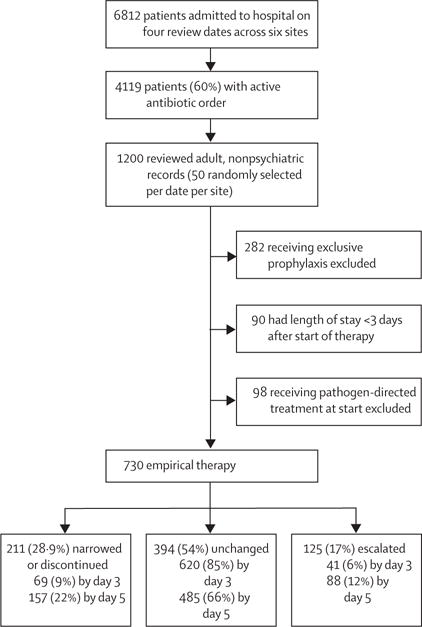
Findings: Across the six study sites, 4119 (60%) of 6812 inpatients received antimicrobials. Of 1200 randomly selected patients with active antimicrobials, 730 (61%) met inclusion criteria. At the start of therapy, 220 (30%) patients were afebrile and had normal white blood cell counts. Appropriate cultures were collected from 432 (59%) patients, and 250 (58%) were negative. By the 5th day of therapy, 12·5% of empirical antimicrobials were escalated, 21·5% were narrowed or discontinued, and 66·4% were unchanged. Narrowing or discontinuation was more likely when cultures were collected at the start of therapy (adjusted OR 1·68, 95% CI 1·05-2·70) and no infection was noted on an initial radiological study (1·76, 1·11-2·79). Escalation was associated with multiple infection sites (2·54, 1·34-4·83) and a positive culture (1·99, 1·20-3·29).
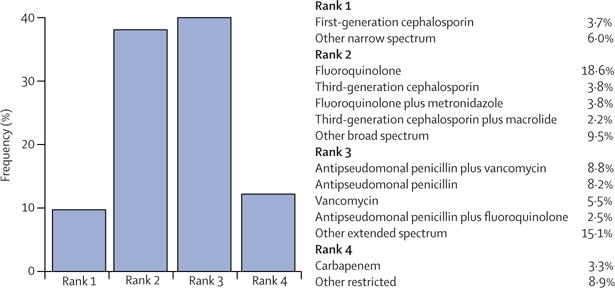
Interpretation: Broad-spectrum empirical therapy is common, even when clinical signs of infection are absent. Fewer than one in three inpatients have their regimens narrowed within 5 days of starting empirical antimicrobials. Improved diagnostic methods and continued education are needed to guide discontinuation of antimicrobials.
Funding: US Centers for Disease Control and Prevention, Division of Healthcare Quality Promotion; Robert Wood Johnson Foundation; US Department of Veterans Administration; US Department of Homeland Security.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
DJM is a research consultant for Sanogiene and Welch Allyn (not related to this work). ES is a member of a 3-M medical advisory board and Sage’s speaker’s bureau (not related to this work). All other authors have no competing interests.
Figures
Comment in
-
Is it time for an antibiotic prenuptial agreement?Lancet Infect Dis. 2014 Dec;14(12):1168-9. doi: 10.1016/S1473-3099(14)70992-2. Epub 2014 Nov 17. Lancet Infect Dis. 2014. PMID: 25455971 No abstract available.
References
-
- Cosgrove SE. The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs. Clin Infect Dis. 2006;42(suppl 2):S82–89. - PubMed
-
- Goossens H, Ferech M, Vander Stichele R, Elseviers M. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365:579–87. - PubMed
-
- Centers for Disease Control and Prevention. CDC’s campaign to prevent antimicrobial resistance in health—care settings. MMWR Morb Mortal Wkly Rep. 2002;51:343. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
