

Noncardiac comorbidities in heart failure with reduced versus preserved ejection fraction
- PMID: 25456761
- PMCID: PMC4254505
- DOI: 10.1016/j.jacc.2014.08.036
Noncardiac comorbidities in heart failure with reduced versus preserved ejection fraction
Abstract
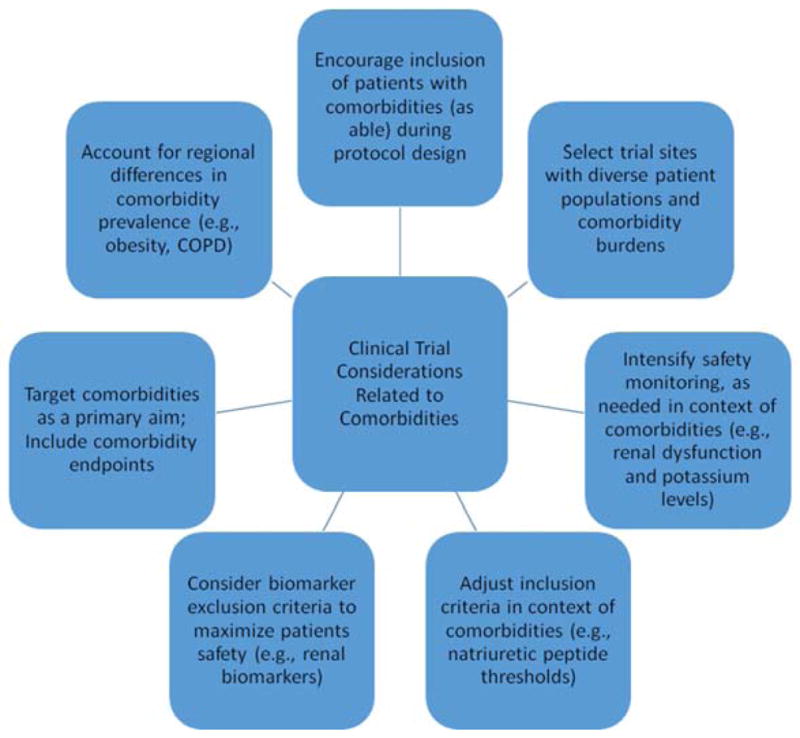
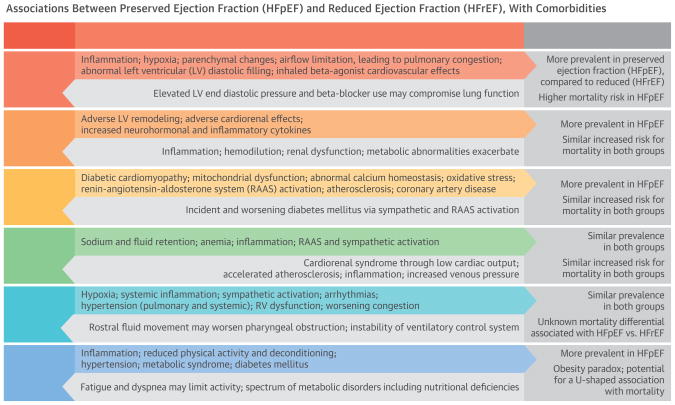
Heart failure patients are classified by ejection fraction (EF) into distinct groups: heart failure with preserved ejection fraction (HFpEF) or heart failure with reduced ejection fraction (HFrEF). Although patients with heart failure commonly have multiple comorbidities that complicate management and may adversely affect outcomes, their role in the HFpEF and HFrEF groups is not well-characterized. This review summarizes the role of noncardiac comorbidities in patients with HFpEF versus HFrEF, emphasizing prevalence, underlying pathophysiologic mechanisms, and outcomes. Pulmonary disease, diabetes mellitus, anemia, and obesity tend to be more prevalent in HFpEF patients, but renal disease and sleep-disordered breathing burdens are similar. These comorbidities similarly increase morbidity and mortality risk in HFpEF and HFrEF patients. Common pathophysiologic mechanisms include systemic and endomyocardial inflammation with fibrosis. We also discuss implications for clinical care and future HF clinical trial design. The basis for this review was discussions between scientists, clinical trialists, and regulatory representatives at the 10th Global CardioVascular Clinical Trialists Forum.
Keywords: comorbidities; ejection fraction; heart failure.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Yancy CW, Lopatin M, Stevenson LW, et al. ADHERE Scientific Advisory Committee and Investigators. Clinical presentation, management, and inhospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: a report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database. J Am Coll Cardiol. 2006;47:76–84. - PubMed
-
- Centers for Medicare and Medicaid Services. Chronic Conditions Among Medicare Beneficiaries. Chartbook, 2012. Baltimore, MD: 2012.
-
- van Deursen VM, Urso R, Laroche C, et al. Co-morbidities in patients with heart failure: an analysis of the European Heart Failure Pilot Survey. Eur J Heart Fail. 2014;16:103–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
