

Relation of dyspnea severity on admission for acute heart failure with outcomes and costs
- PMID: 25456875
- PMCID: PMC4262730
- DOI: 10.1016/j.amjcard.2014.09.048
Relation of dyspnea severity on admission for acute heart failure with outcomes and costs
Abstract
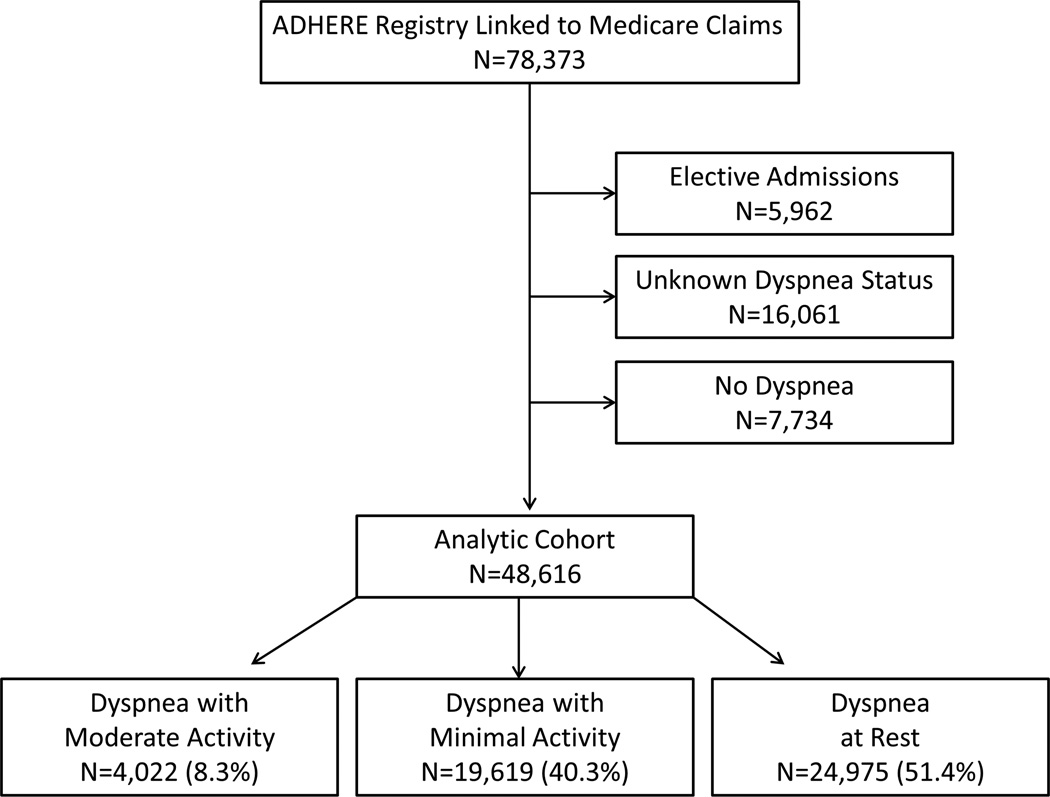
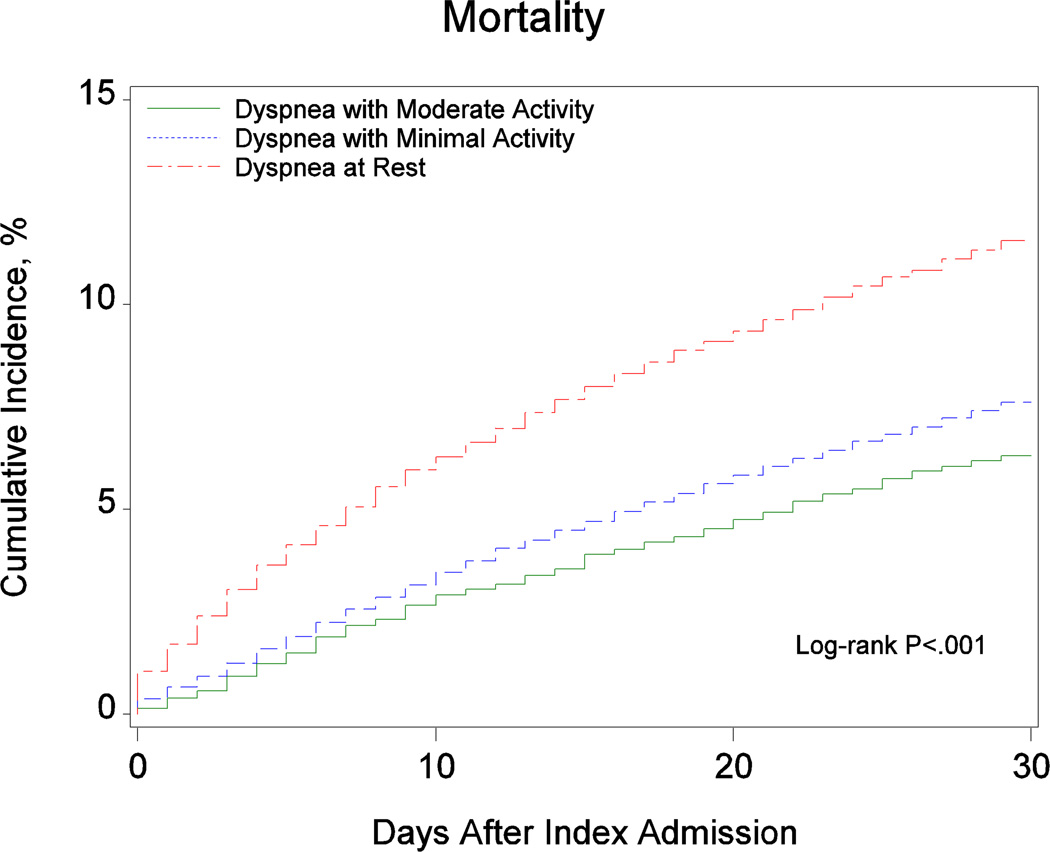
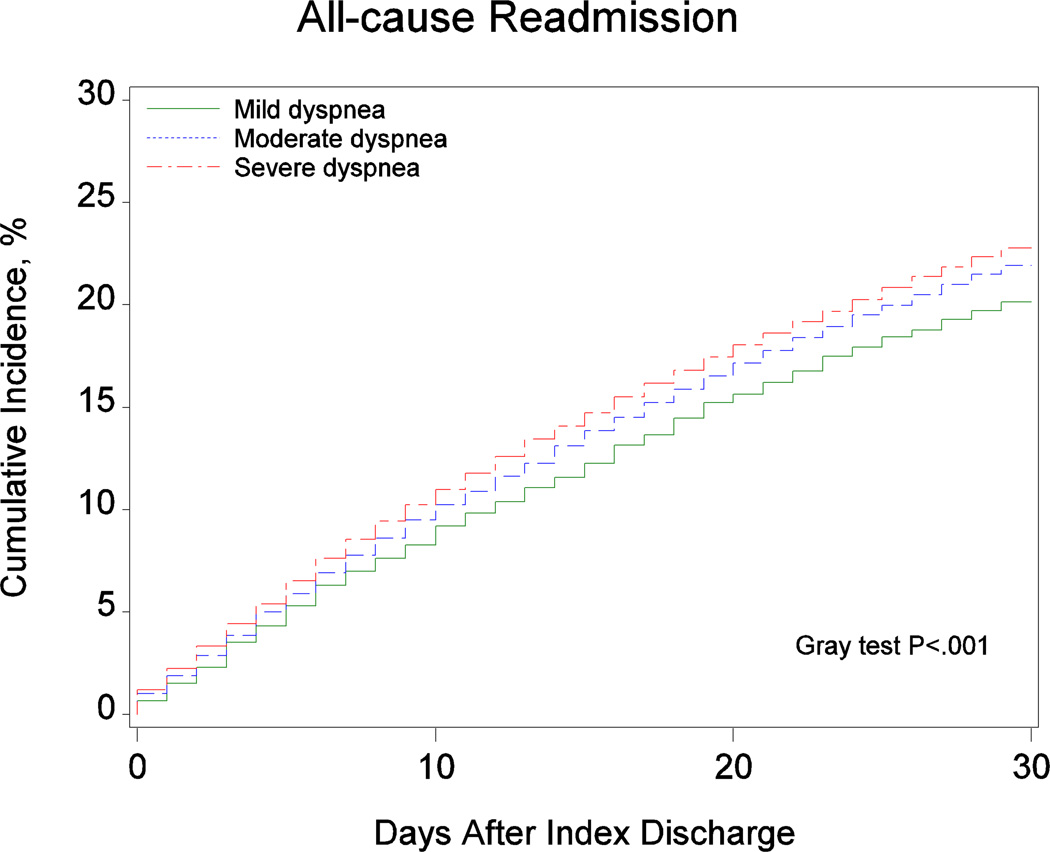
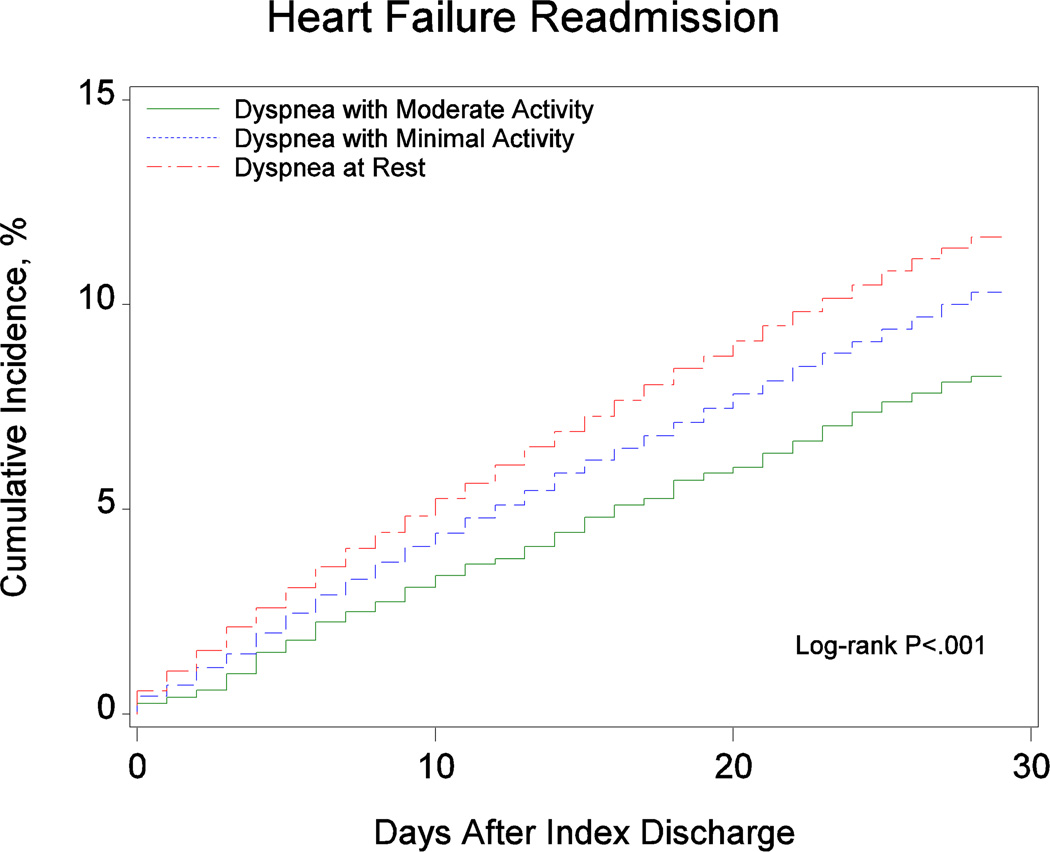
Hospitalization for heart failure (HF) is frequently related to dyspnea, yet associations among dyspnea severity, outcomes, and health care costs are unknown. The aim of this study was to describe the characteristics of patients hospitalized for acute HF by dyspnea severity and to examine associations among dyspnea severity, outcomes, and costs. Registry data for patients hospitalized for HF were linked with Medicare claims to evaluate dyspnea and outcomes in patients ≥65 years of age. We classified patients by patient-reported dyspnea severity at admission. Outcomes included length of stay, mortality 30 days after admission, days alive and out of the hospital, readmission, and Medicare payments 30 days after discharge. Of 48,616 patients with acute HF and dyspnea, 4,022 (8.3%) had dyspnea with moderate activity, 19,619 (40.3%) with minimal activity, and 24,975 (51.4%) at rest. Patients with dyspnea with minimal activity or at rest had greater co-morbidities, including renal insufficiency. Greater severity of baseline dyspnea was associated with mortality (moderate activity, 6.3%; minimal activity, 7.6%; at rest, 11.6%) and HF readmission (7.2%, 9.0%, and 9.4%). After multivariate adjustment, dyspnea at rest was associated with greater 30-day mortality and HF readmission, fewer days alive and out of the hospital, longer length of stay, and higher Medicare payments compared with dyspnea with moderate activity. In conclusion, dyspnea at rest on presentation was associated with greater mortality, readmission, length of stay, and health care costs in patients hospitalized with acute HF.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Executive summary: heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127:143–152. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e147–e239. - PubMed
-
- Braunschweig F, Cowie MR, Auricchio A. What are the costs of heart failure? Europace. 2011;13(Suppl 2):ii13–ii17. - PubMed
-
- Gheorghiade M, Zannad F, Sopko G, Klein L, Piña IL, Konstam MA, Massie BM, Roland E, Targum S, Collins SP, Filippatos G, Tavazzi L. Acute heart failure syndromes: current state and framework for future research. Circulation. 2005;112:3958–3968. - PubMed
-
- Mentz RJ, Hernandez AF, Stebbins A, Ezekowitz JA, Felker GM, Heizer GM, Atar D, Teerlink JR, Califf RM, Massie BM, Hasselblad V, Starling RC, O'Connor CM, Ponikowski P. Predictors of early dyspnoea relief in acute heart failure and the association with 30-day outcomes: findings from ASCEND-HF. Eur J Heart Fail. 2013;15:456–464. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
