

Inflammation, metabolic dysregulation, and pulmonary function among obese urban adolescents with asthma
- PMID: 25457349
- PMCID: PMC4347436
- DOI: 10.1164/rccm.201409-1587OC
Inflammation, metabolic dysregulation, and pulmonary function among obese urban adolescents with asthma
Abstract
Rationale: Insulin resistance and low high-density lipoprotein (HDL) are associated with pulmonary morbidity, including asthma, but the underlying mechanisms are not well elucidated.
Objectives: To investigate whether systemic inflammation underlies the association of metabolic abnormalities with pulmonary function among urban adolescents.
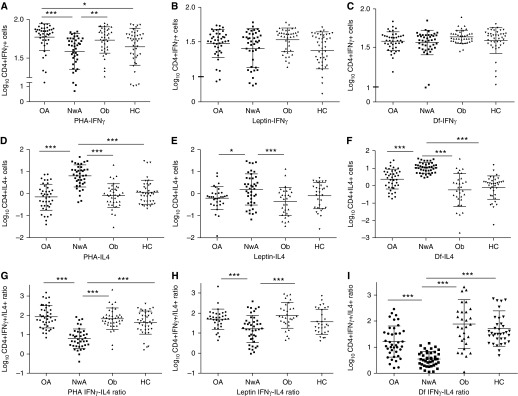
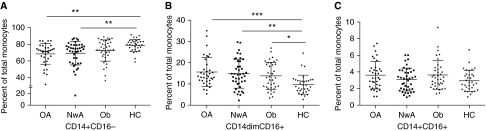
Methods: Th-cell responses and monocyte subsets, and their association with serum homeostatic model assessment of insulin resistance (HOMA-IR) and HDL, and pulmonary function were quantified in 168 adolescents, including 42 obese subjects with asthma, 42 normal-weight subjects with asthma, 40 obese subjects without asthma, and 44 healthy control subjects. Th-cell responses (Th1 [CD4(+)IFNγ(+)] and Th2 [CD4(+)IL4(+)] cells) to stimulation with phytohemagglutinin, leptin, and dust mite, and classical (CD14(+)CD16(-)), resident (CD14(+)CD16(+)), and patrolling (CD14dimCD16(+)) monocytes, and their C-C chemokine receptor type-2 (CCR2) expression were quantified by flow cytometry.
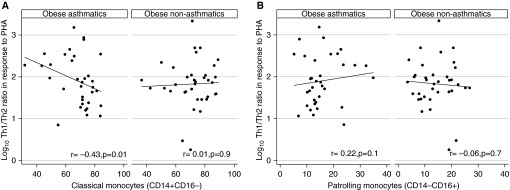
Measurements and main results: Th1/Th2 ratio to all three stimuli was higher in obese subjects with asthma than normal-weight subjects with asthma and directly correlated with HOMA-IR. Classical monocytes inversely associated with Th1/Th2 ratio to phytohemagglutinin (r = -0.43; P = 0.01) and directly with Asthma Control Test score (β = 1.09; P = 0.04), while patrolling monocytes correlated with Composite Asthma Severity Index score (β = 1.11; P = 0.04) only among obese subjects with asthma. HDL was inversely associated with patrolling monocytes and directly associated with CCR2 expression on resident monocytes. CCR2 expression on patrolling monocytes predicted residual volume (RV), RV/TLC ratio, and FRC, after adjusting for HDL, but not after adjusting for body mass index. Association of Th1/Th2 ratio with RV, FRC, and inspiratory capacity was attenuated after adjusting for HOMA-IR.
Conclusions: Th1 polarization and monocyte activation among obese subjects with asthma correlates with metabolic abnormalities. Association of monocyte activation with pulmonary function is mediated by body mass index, whereas that of Th1 polarization is mediated by insulin resistance.
Keywords: asthma; inflammation; metabolic dysregulation; obesity; pulmonary function.
Figures
Comment in
-
Metabolic dysregulation. Driving the obese asthma phenotype in adolescents?Am J Respir Crit Care Med. 2015 Jan 15;191(2):121-2. doi: 10.1164/rccm.201412-2221ED. Am J Respir Crit Care Med. 2015. PMID: 25590150 No abstract available.
References
-
- Gold DR, Damokosh AI, Dockery DW, Berkey CS. Body-mass index as a predictor of incident asthma in a prospective cohort of children. Pediatr Pulmonol. 2003;36:514–521. - PubMed
-
- Lang JE, Hossain J, Smith K, Lima JJ. Asthma severity, exacerbation risk, and controller treatment burden in underweight and obese children. J Asthma. 2012;49:456–463. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
