

Development and validation of a seizure prediction model in critically ill children
- PMID: 25458097
- PMCID: PMC4315714
- DOI: 10.1016/j.seizure.2014.09.013
Development and validation of a seizure prediction model in critically ill children
Abstract
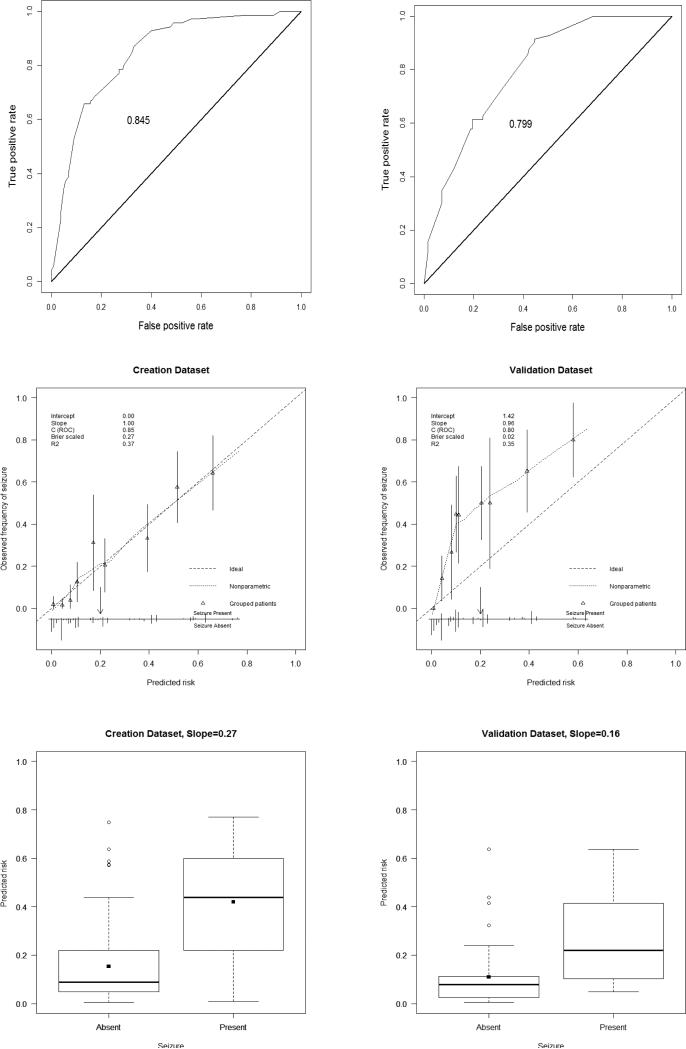
Purpose: Electrographic seizures are common in encephalopathic critically ill children, but identification requires continuous EEG monitoring (CEEG). Development of a seizure prediction model would enable more efficient use of limited CEEG resources. We aimed to develop and validate a seizure prediction model for use among encephalopathic critically ill children.
Method: We developed a seizure prediction model using a retrospectively acquired multi-center database of children with acute encephalopathy without an epilepsy diagnosis, who underwent clinically indicated CEEG. We performed model validation using a separate prospectively acquired single center database. Predictor variables were chosen to be readily available to clinicians prior to the onset of CEEG and included: age, etiology category, clinical seizures prior to CEEG, initial EEG background category, and inter-ictal discharge category.
Results: The model has fair to good discrimination ability and overall performance. At the optimal cut-off point in the validation dataset, the model has a sensitivity of 59% and a specificity of 81%. Varied cut-off points could be chosen to optimize sensitivity or specificity depending on available CEEG resources.
Conclusion: Despite inherent variability between centers, a model developed using multi-center CEEG data and few readily available variables could guide the use of limited CEEG resources when applied at a single center. Depending on CEEG resources, centers could choose lower cut-off points to maximize identification of all patients with seizures (but with more patients monitored) or higher cut-off points to reduce resource utilization by reducing monitoring of lower risk patients (but with failure to identify some patients with seizures).
Keywords: EEG monitoring; Non-convulsive seizure; Pediatric; Prediction model; Seizure; Status epilepticus.
Copyright © 2014 British Epilepsy Association. Published by Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Development of a model to predict electroencephalographic seizures in critically ill children.Epilepsia. 2020 Mar;61(3):498-508. doi: 10.1111/epi.16448. Epub 2020 Feb 20. Epilepsia. 2020. PMID: 32077099
-
Validation of a model to predict electroencephalographic seizures in critically ill children.Epilepsia. 2020 Dec;61(12):2754-2762. doi: 10.1111/epi.16724. Epub 2020 Oct 16. Epilepsia. 2020. PMID: 33063870
-
Electroencephalography monitoring in critically ill children: current practice and implications for future study design.Epilepsia. 2013 Aug;54(8):1419-27. doi: 10.1111/epi.12261. Epub 2013 Jul 12. Epilepsia. 2013. PMID: 23848569 Free PMC article.
-
Detection of electrographic seizures with continuous EEG monitoring in critically ill patients.Neurology. 2004 May 25;62(10):1743-8. doi: 10.1212/01.wnl.0000125184.88797.62. Neurology. 2004. PMID: 15159471 Review.
-
Continuous Electroencephalography Monitoring in Critically Ill Infants and Children.Pediatr Neurol. 2020 Jul;108:40-46. doi: 10.1016/j.pediatrneurol.2020.04.009. Epub 2020 Apr 26. Pediatr Neurol. 2020. PMID: 32446643 Review.
Cited by
-
Electrographic status epilepticus in children with critical illness: Epidemiology and outcome.Epilepsy Behav. 2015 Aug;49:223-7. doi: 10.1016/j.yebeh.2015.03.007. Epub 2015 May 2. Epilepsy Behav. 2015. PMID: 25944114 Free PMC article. Review.
-
Seizure Prediction Models in the Neonatal Intensive Care Unit.J Clin Neurophysiol. 2019 May;36(3):186-194. doi: 10.1097/WNP.0000000000000574. J Clin Neurophysiol. 2019. PMID: 30882530 Free PMC article.
-
Association of EEG characteristics with outcomes following pediatric ICU cardiac arrest: A secondary analysis of the ICU-RESUScitation trial.Resuscitation. 2024 Aug;201:110271. doi: 10.1016/j.resuscitation.2024.110271. Epub 2024 Jun 10. Resuscitation. 2024. PMID: 38866233 Free PMC article. Clinical Trial.
-
Validation of a Model for Targeted EEG Monitoring Duration in Critically Ill Children.J Clin Neurophysiol. 2023 Nov 1;40(7):589-599. doi: 10.1097/WNP.0000000000000940. Epub 2022 Apr 20. J Clin Neurophysiol. 2023. PMID: 35512186 Free PMC article.
-
Real-time seizure detection in paediatric intensive care patients: the RESET child brain protocol.BMJ Open. 2022 Jun 3;12(6):e059301. doi: 10.1136/bmjopen-2021-059301. BMJ Open. 2022. PMID: 36691237 Free PMC article.
References
-
- Abend NS, Wusthoff CJ, Goldberg EM, Dlugos DJ. Electrographic seizures and status epilepticus in critically ill children and neonates with encephalopathy. Lancet Neurol. 2013;12:1170–9. - PubMed
-
- Hosain SA, Solomon GE, Kobylarz EJ. Electroencephalographic patterns in unresponsive pediatric patients. Pediatr Neurol. 2005;32:162–5. - PubMed
-
- Jette N, Claassen J, Emerson RG, Hirsch LJ. Frequency and predictors of nonconvulsive seizures during continuous electroencephalographic monitoring in critically ill children. Arch Neurol. 2006;63:1750–5. - PubMed
-
- Abend NS, Dlugos DJ. Nonconvulsive status epilepticus in a pediatric intensive care unit. Pediatr Neurol. 2007;37:165–70. - PubMed
-
- Tay SK, Hirsch LJ, Leary L, Jette N, Wittman J, Akman CI. Nonconvulsive status epilepticus in children: clinical and EEG characteristics. Epilepsia. 2006;47:1504–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
