

A population-based, multifaceted strategy to implement antenatal corticosteroid treatment versus standard care for the reduction of neonatal mortality due to preterm birth in low-income and middle-income countries: the ACT cluster-randomised trial
- PMID: 25458726
- PMCID: PMC4420619
- DOI: 10.1016/S0140-6736(14)61651-2
A population-based, multifaceted strategy to implement antenatal corticosteroid treatment versus standard care for the reduction of neonatal mortality due to preterm birth in low-income and middle-income countries: the ACT cluster-randomised trial
Abstract
Background: Antenatal corticosteroids for pregnant women at risk of preterm birth are among the most effective hospital-based interventions to reduce neonatal mortality. We aimed to assess the feasibility, effectiveness, and safety of a multifaceted intervention designed to increase the use of antenatal corticosteroids at all levels of health care in low-income and middle-income countries.
Methods: In this 18-month, cluster-randomised trial, we randomly assigned (1:1) rural and semi-urban clusters within six countries (Argentina, Guatemala, India, Kenya, Pakistan, and Zambia) to standard care or a multifaceted intervention including components to improve identification of women at risk of preterm birth and to facilitate appropriate use of antenatal corticosteroids. The primary outcome was 28-day neonatal mortality among infants less than the 5th percentile for birthweight (a proxy for preterm birth) across the clusters. Use of antenatal corticosteroids and suspected maternal infection were additional main outcomes. This trial is registered with ClinicalTrials.gov, number NCT01084096.
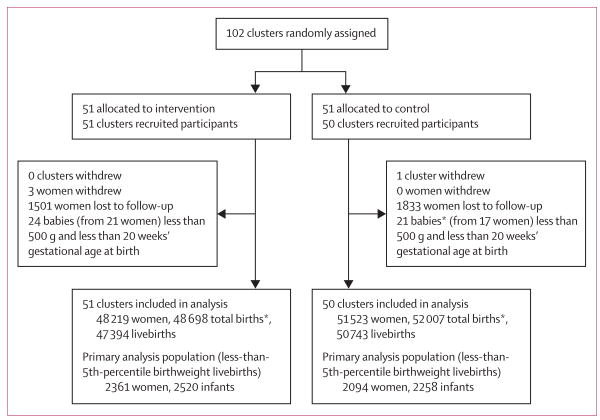
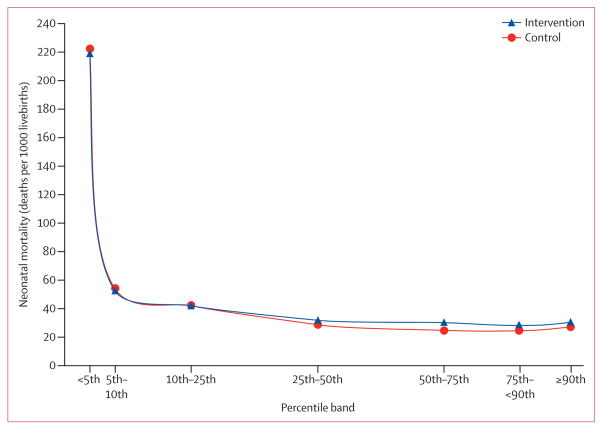
Findings: The ACT trial took place between October, 2011, and March, 2014 (start dates varied by site). 51 intervention clusters with 47,394 livebirths (2520 [5%] less than 5th percentile for birthweight) and 50 control clusters with 50,743 livebirths (2258 [4%] less than 5th percentile) completed follow-up. 1052 (45%) of 2327 women in intervention clusters who delivered less-than-5th-percentile infants received antenatal corticosteroids, compared with 215 (10%) of 2062 in control clusters (p<0·0001). Among the less-than-5th-percentile infants, 28-day neonatal mortality was 225 per 1000 livebirths for the intervention group and 232 per 1000 livebirths for the control group (relative risk [RR] 0·96, 95% CI 0·87-1·06, p=0·65) and suspected maternal infection was reported in 236 (10%) of 2361 women in the intervention group and 133 (6%) of 2094 in the control group (odds ratio [OR] 1·67, 1·33-2·09, p<0·0001). Among the whole population, 28-day neonatal mortality was 27·4 per 1000 livebirths for the intervention group and 23·9 per 1000 livebirths for the control group (RR 1·12, 1·02-1·22, p=0·0127) and suspected maternal infection was reported in 1207 (3%) of 48,219 women in the intervention group and 867 (2%) of 51,523 in the control group (OR 1·45, 1·33-1·58, p<0·0001).
Interpretation: Despite increased use of antenatal corticosteroids in low-birthweight infants in the intervention groups, neonatal mortality did not decrease in this group, and increased in the population overall. For every 1000 women exposed to this strategy, an excess of 3·5 neonatal deaths occurred, and the risk of maternal infection seems to have been increased.
Funding: Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Scaling up antenatal corticosteroids in low-resource settings?Lancet. 2015 Feb 14;385(9968):585-587. doi: 10.1016/S0140-6736(14)61699-8. Epub 2014 Oct 15. Lancet. 2015. PMID: 25458729 No abstract available.
-
Antenatal corticosteroids for preterm births in resource-limited settings.Lancet. 2015 May 16;385(9981):1943-4. doi: 10.1016/S0140-6736(15)60953-9. Lancet. 2015. PMID: 26090635 No abstract available.
-
Antenatal corticosteroids for preterm births in resource-limited settings.Lancet. 2015 May 16;385(9981):1944. doi: 10.1016/S0140-6736(15)60954-0. Lancet. 2015. PMID: 26090636 No abstract available.
-
Antenatal corticosteroids for preterm births in resource-limited settings.Lancet. 2015 May 16;385(9981):1944-5. doi: 10.1016/S0140-6736(15)60955-2. Lancet. 2015. PMID: 26090637 No abstract available.
-
Antenatal corticosteroids for preterm births in resource-limited settings - Authors' reply.Lancet. 2015 May 16;385(9981):1945. doi: 10.1016/S0140-6736(15)60956-4. Lancet. 2015. PMID: 26090638 No abstract available.
-
One Simple Intervention Begets Another: Let's Get the Gestational Age Right First.Matern Child Health J. 2016 Sep;20(9):1767-8. doi: 10.1007/s10995-016-2003-3. Matern Child Health J. 2016. PMID: 27146397 No abstract available.
References
-
- National Institutes of Health. The effect of corticosteroids for fetal maturation on perinatal outcomes. Consensus Development Conference Statement; Feb 28–March 2, 1994; [accessed June 1, 2014]. http://consensus.nih.gov/1994/1994AntenatalSteroidPerinatal095html.htm. - PubMed
-
- Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006;3:CD004454. - PubMed
-
- Lawn JE, Blencowe H, Oza S, et al. for The Lancet Every Newborn Study Group Every Newborn: progress, priorities, and potential beyond survival. Lancet. 2014;384:189–205. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 HD058326/HD/NICHD NIH HHS/United States
- UG1 HD076461/HD/NICHD NIH HHS/United States
- K24 AT003683/AT/NCCIH NIH HHS/United States
- U01 HD040607/HD/NICHD NIH HHS/United States
- U01 HD040657/HD/NICHD NIH HHS/United States
- D43 TW009083/TW/FIC NIH HHS/United States
- U01 HD042372/HD/NICHD NIH HHS/United States
- U01 HD040636/HD/NICHD NIH HHS/United States
- U01 HD040477/HD/NICHD NIH HHS/United States
- U10 HD078437/HD/NICHD NIH HHS/United States
- U01 HD058322/HD/NICHD NIH HHS/United States
- U24 HD092094/HD/NICHD NIH HHS/United States
- U01 HD043464/HD/NICHD NIH HHS/United States
- U10 HD076461/HD/NICHD NIH HHS/United States
- U10 HD076457/HD/NICHD NIH HHS/United States
- UG1 HD076474/HD/NICHD NIH HHS/United States
- U10 HD076474/HD/NICHD NIH HHS/United States
- U10 HD078439/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
