

Atopic dermatitis in children: clinical features, pathophysiology, and treatment
- PMID: 25459583
- PMCID: PMC4254569
- DOI: 10.1016/j.iac.2014.09.008
Atopic dermatitis in children: clinical features, pathophysiology, and treatment
Abstract
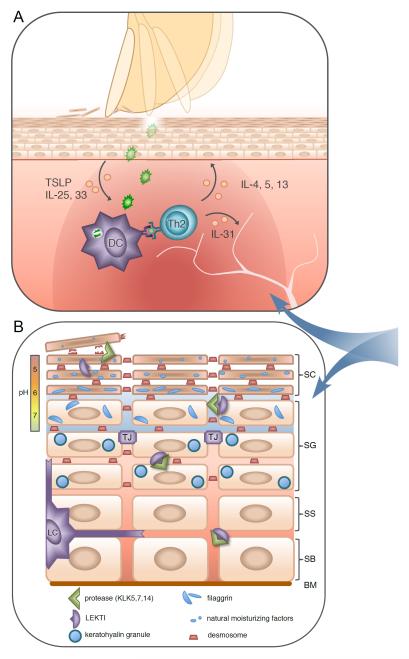
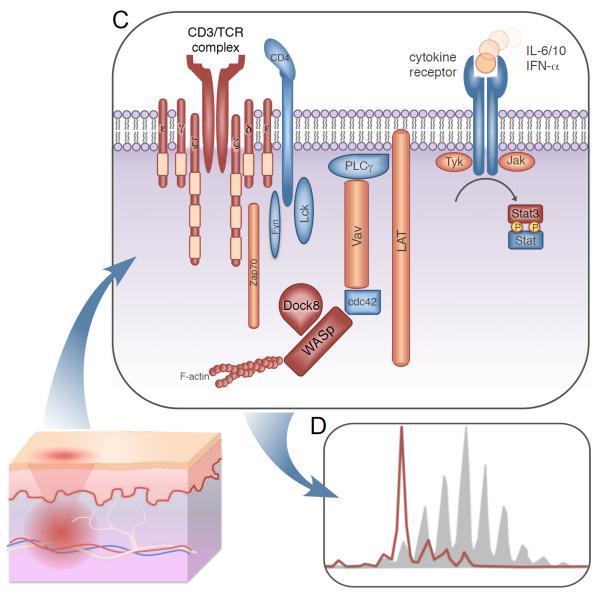
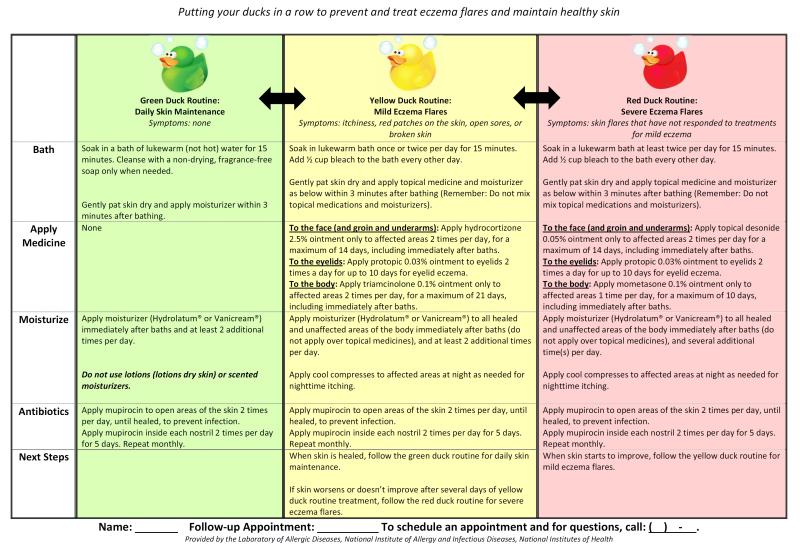
Atopic dermatitis (AD) is a chronic, relapsing, highly pruritic skin condition resulting from disruption of the epithelial barrier and associated immune dysregulation in the skin of genetically predisposed hosts. AD generally develops in early childhood, has a characteristic age-dependent distribution and is commonly associated with elevated IgE, peripheral eosinophilia, and other allergic diseases. Medications such as antihistamines have demonstrated poor efficacy in controlling AD-associated itch. Education of patients regarding the primary underlying defects and provision of a comprehensive skin care plan is essential for disease maintenance and management of flares.
Keywords: Allergy; Atopic dermatitis; Eczema; Hyper-IgE syndrome; Netherton syndrome.
Published by Elsevier Inc.
Figures

References
-
- Williams H, Robertson C, Stewart A, Ait-Khaled N, Anabwani G, Anderson R, et al. Worldwide variations in the prevalence of symptoms of atopic eczema in the International Study of Asthma and Allergies in Childhood. The Journal of allergy and clinical immunology. 1999 Jan;103(1 Pt 1):125–38. PubMed PMID: 9893196. - PubMed
-
- Flohr C, Johansson SG, Wahlgren CF, Williams H. How atopic is atopic dermatitis? The Journal of allergy and clinical immunology. 2004 Jul;114(1):150–8. PubMed PMID: 15241359. - PubMed
-
- Fleischer DM, Bock SA, Spears GC, Wilson CG, Miyazawa NK, Gleason MC, et al. Oral food challenges in children with a diagnosis of food allergy. The Journal of pediatrics. 2011 Apr;158(4):578–83. e1. PubMed PMID: 21030035. - PubMed
-
- Paller AS, McAlister RO, Doyle JJ, Jackson A. Perceptions of physicians and pediatric patients about atopic dermatitis, its impact, and its treatment. Clinical pediatrics. 2002 Jun;41(5):323–32. PubMed PMID: 12086198. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
