

Strategies for the identification of T cell-recognized tumor antigens in hematological malignancies for improved graft-versus-tumor responses after allogeneic blood and marrow transplantation
- PMID: 25459643
- PMCID: PMC4426024
- DOI: 10.1016/j.bbmt.2014.11.001
Strategies for the identification of T cell-recognized tumor antigens in hematological malignancies for improved graft-versus-tumor responses after allogeneic blood and marrow transplantation
Abstract
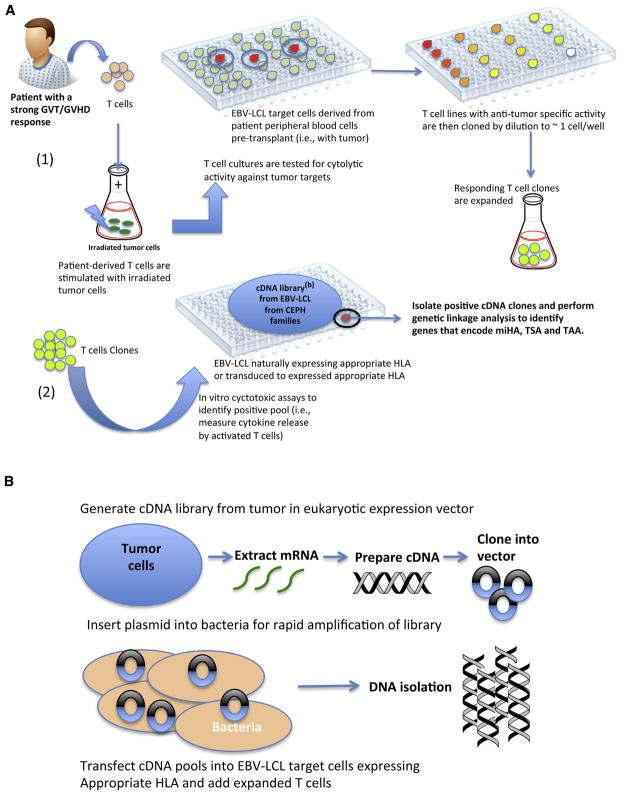
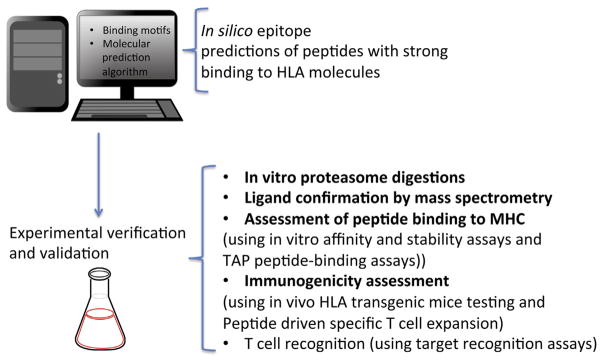
Allogeneic blood and marrow transplantation (allo-BMT) is an effective immunotherapeutic treatment that can provide partial or complete remission for patients with hematological malignancies. Mature donor T cells in the donor inoculum play a central role in mediating graft-versus-tumor (GVT) responses by destroying residual tumor cells that persist after conditioning regimens. Alloreactivity towards minor histocompatibility antigens (miHA), which are varied tissue-related self-peptides presented in the context of major histocompatibility complex (MHC) molecules on recipient cells, some of which may be shared on tumor cells, is a dominant factor for the development of GVT. Potentially, GVT can also be directed to tumor-associated antigens or tumor-specific antigens that are more specific to the tumor cells themselves. The full exploitation of allo-BMT, however, is greatly limited by the development of graft-versus-host disease (GVHD), which is mediated by the donor T cell response against the miHA expressed in the recipient's cells of the intestine, skin, and liver. Because of the significance of GVT and GVHD responses in determining the clinical outcome of patients, miHA and tumor antigens have been intensively studied, and one active immunotherapeutic approach to separate these two responses has been cancer vaccination after allo-BMT. The combination of these two strategies has an advantage over vaccination of the patient without allo-BMT because his or her immune system has already been exposed and rendered unresponsive to the tumor antigens. The conditioning for allo-BMT eliminates the patient's existing immune system, including regulatory elements, and provides a more permissive environment for the newly developing donor immune compartment to selectively target the malignant cells. Utilizing recent technological advances, the identities of many human miHA and tumor antigenic peptides have been defined and are currently being evaluated in clinical and basic immunological studies for their ability to produce effective T cell responses. The first step towards this goal is the identification of targetable tumor antigens. In this review, we will highlight some of the technologies currently used to identify tumor antigens and anti-tumor T cell clones in hematological malignancies.
Keywords: Blood and marrow transplantation; Hematological malignancy; Minor histocompatibility antigens; Tumor vaccination; Tumor-associated antigens; Tumor-specific antigens.
Copyright © 2015 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest statement: There are no conflicts of interest to report.
Figures
References
-
- Luznik L, Fuchs EJ. Donor lymphocyte infusions to treat hematologic malignancies in relapse after allogeneic blood or marrow transplantation. Cancer Control. 2002;9:123–137. - PubMed
-
- Kolb HJ, Simoes B, Schmid C. Cellular immunotherapy after allogeneic stem cell transplantation in hematologic malignancies. Curr Opin Oncol. 2004;16:167–173. - PubMed
-
- Zorn E, Wang KS, Hochberg EP, et al. Infusion of CD4+ donor lymphocytes induces the expansion of CD8+ donor T cells with cytolytic activity directed against recipient hematopoietic cells. Clin Cancer Res. 2002;8:2052–2060. - PubMed
-
- Alyea EP, DeAngelo DJ, Moldrem J, et al. NCI First International Workshop on The Biology, Prevention and Treatment of Relapse after Allogeneic Hematopoietic Cell Transplantation: report from the committee on prevention of relapse following allogeneic cell transplantation for hematologic malignancies. Biol Blood Marrow Transplant. 2010;16:1037–1069. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
