

Iron supplementation and mortality in incident dialysis patients: an observational study
- PMID: 25462819
- PMCID: PMC4252084
- DOI: 10.1371/journal.pone.0114144
Iron supplementation and mortality in incident dialysis patients: an observational study
Abstract
Background: Studies on the association between iron supplementation and mortality in dialysis patients are rare and conflicting.
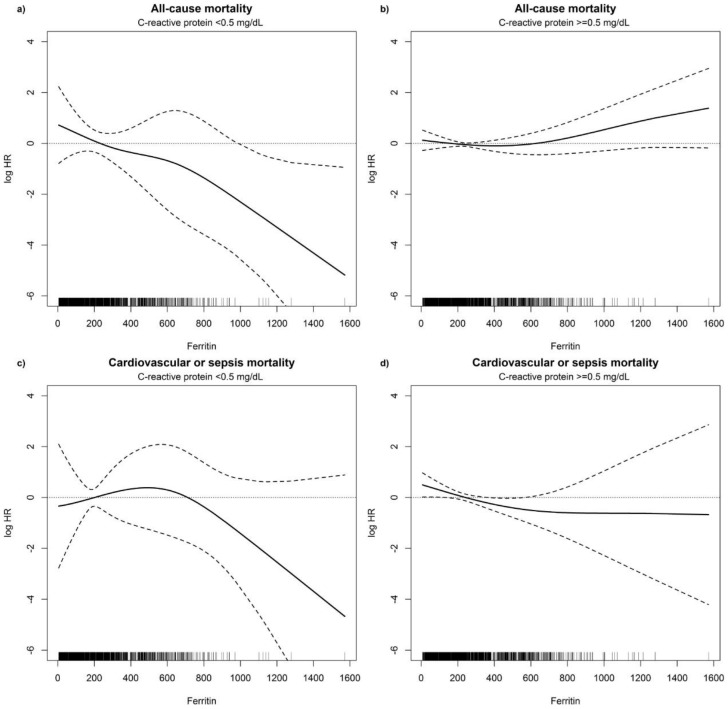
Methods: In our observational single-center cohort study (INVOR study) we prospectively studied 235 incident dialysis patients. Time-dependent Cox proportional hazards models using all measured laboratory values for up to 7.6 years were applied to study the association between iron supplementation and all-cause mortality, cardiovascular and sepsis-related mortality. Furthermore, the time-dependent association of ferritin levels with mortality in patients with normal C-reactive protein (CRP) levels (<0.5 mg/dL) and elevated CRP levels (≧0.5 mg/dL) was evaluated by using non-linear P-splines to allow flexible modeling of the association.
Results: One hundred and ninety-one (81.3%) patients received intravenous iron, 13 (5.5%) patients oral iron, whereas 31 (13.2%) patients were never supplemented with iron throughout the observation period. Eighty-two (35%) patients died during a median follow-up of 34 months, 38 patients due to cardiovascular events and 21 patients from sepsis. Baseline CRP levels were not different between patients with and without iron supplementation. However, baseline serum ferritin levels were lower in patients receiving iron during follow up (median 93 vs 251 ng/mL, p<0.001). Iron supplementation was associated with a significantly reduced all-cause mortality [HR (95%CI): 0.22 (0.08-0.58); p = 0.002] and a reduced cardiovascular and sepsis-related mortality [HR (95%CI): 0.31 (0.09-1.04); p = 0.06]. Increasing ferritin concentrations in patients with normal CRP were associated with a decreasing mortality, whereas in patients with elevated CRP values ferritin levels>800 ng/mL were linked with increased mortality.
Conclusions: Iron supplementation is associated with reduced all-cause mortality in incident dialysis patients. While serum ferritin levels up to 800 ng/mL appear to be safe, higher ferritin levels are associated with increased mortality in the setting of concomitant inflammation.
Conflict of interest statement
Figures

References
-
- Koch KM, Bechstein PB, Fassbinder W, Kaltwasser P, Schoeppe W, et al. (1976) Occult blood loss and iron balance in chronic renal failure. Proc Eur Dial Transplant Assoc 12:362–369. - PubMed
-
- Lindsay RM, Burton JA, King P, Davidson JF, Boddy K, et al. (1973) The measurement of dialyzer blood loss. Clin Nephrol 1:24–28. - PubMed
-
- Goch J, Birgegard G, Danielson BG, Wikstrom B (1996) Iron absorption in patients with chronic uremia on maintenance hemodialysis and in healthy volunteers measured with a simple oral iron load test. Nephron 73:403–406. - PubMed
-
- Eschbach JW, Adamson JW (1999) Iron overload in renal failure patients: changes since the introduction of erythropoietin therapy. Kidney Int Suppl 69: S35–43. - PubMed
-
- Weiss G, Goodnough LT (2005) Anemia of chronic disease. N Engl J Med 352:1011–1023. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
