

Technical complications during veno-venous extracorporeal membrane oxygenation and their relevance predicting a system-exchange--retrospective analysis of 265 cases
- PMID: 25464516
- PMCID: PMC4251903
- DOI: 10.1371/journal.pone.0112316
Technical complications during veno-venous extracorporeal membrane oxygenation and their relevance predicting a system-exchange--retrospective analysis of 265 cases
Abstract
Objectives: Technical complications are a known hazard in veno-venous extracorporeal membrane oxygenation (vvECMO). Identifying these complications and predictive factors indicating a developing system-exchange was the goal of the study.
Methods: Retrospective study on prospectively collected data of technical complications including 265 adult patients (Regensburg ECMO Registry, 2009-2013) with acute respiratory failure treated with vvECMO. Alterations in blood flow resistance, gas transfer capability, hemolysis, coagulation and hemostasis parameters were evaluated in conjunction with a system-exchange in all patients with at least one exchange (n = 83).
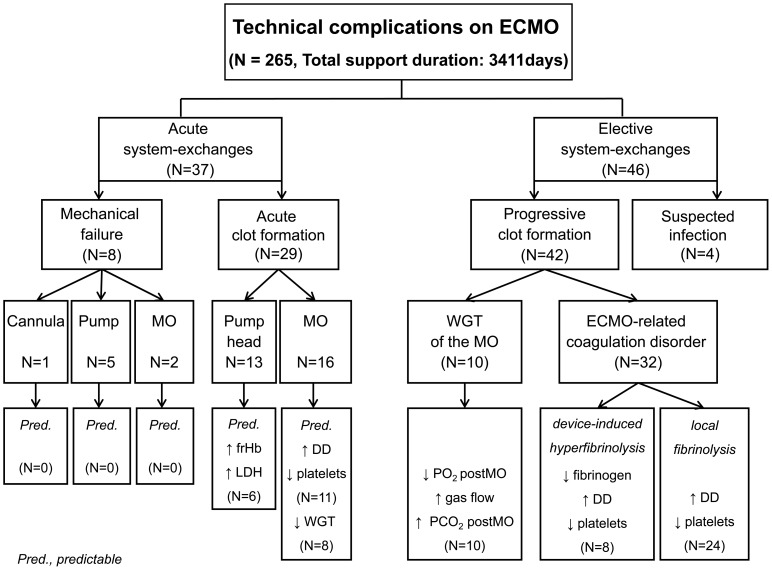
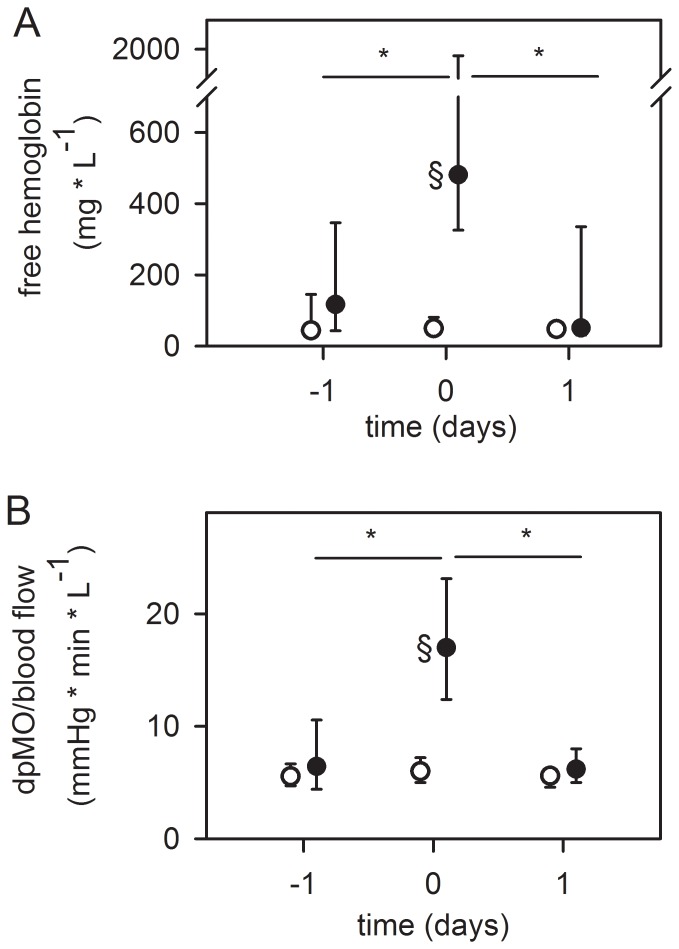
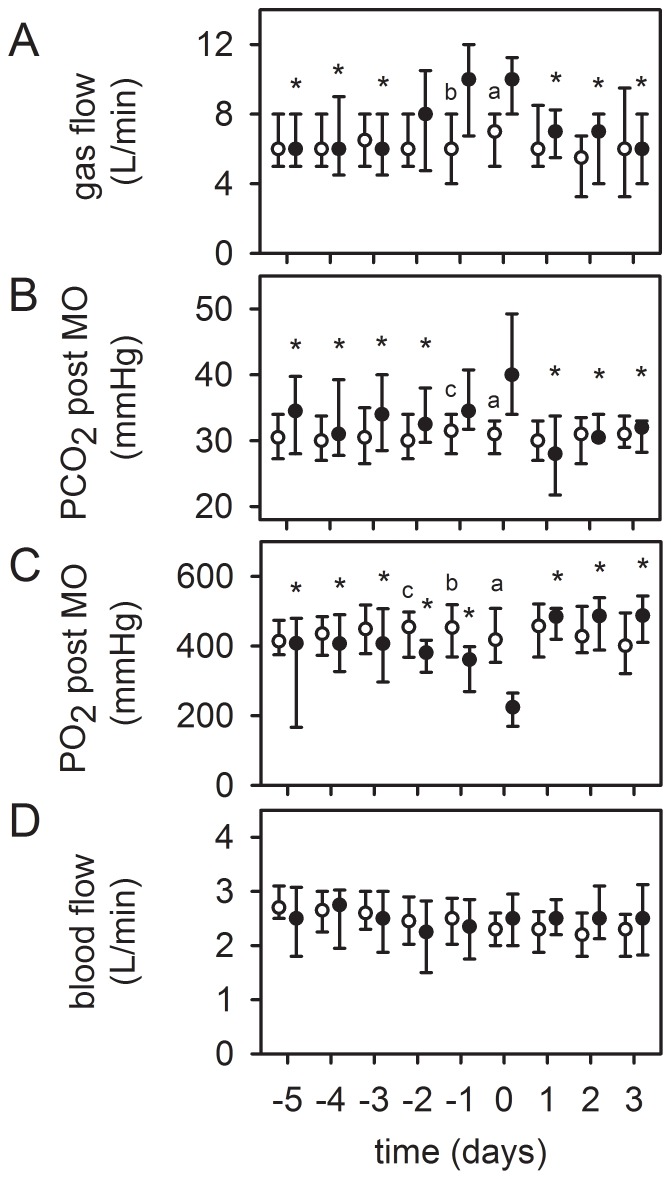
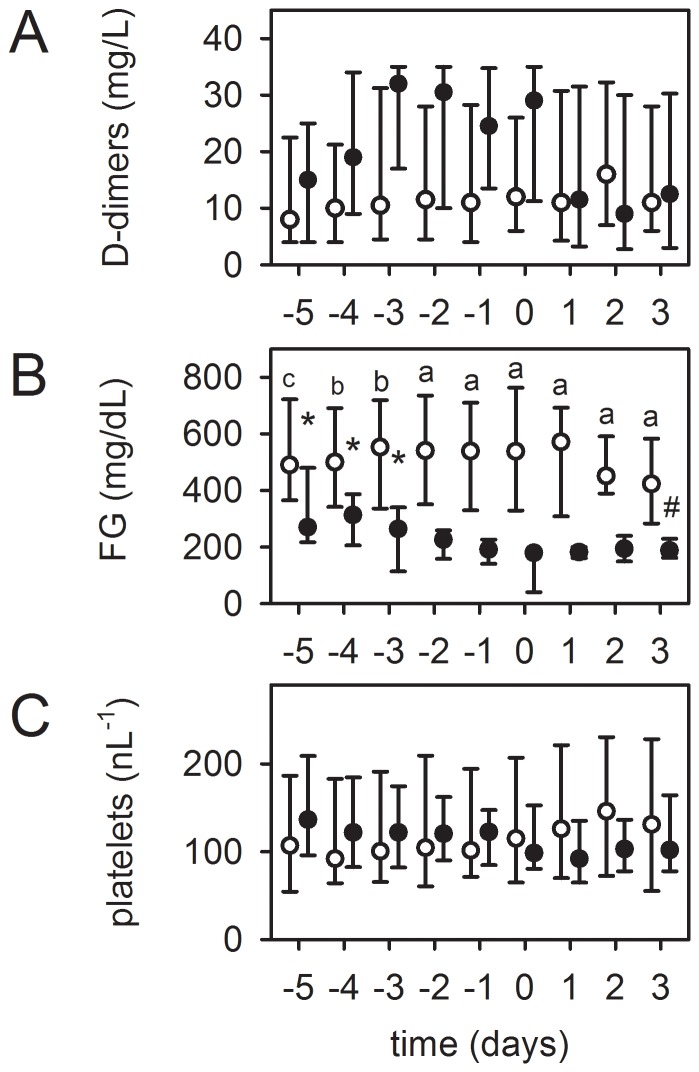
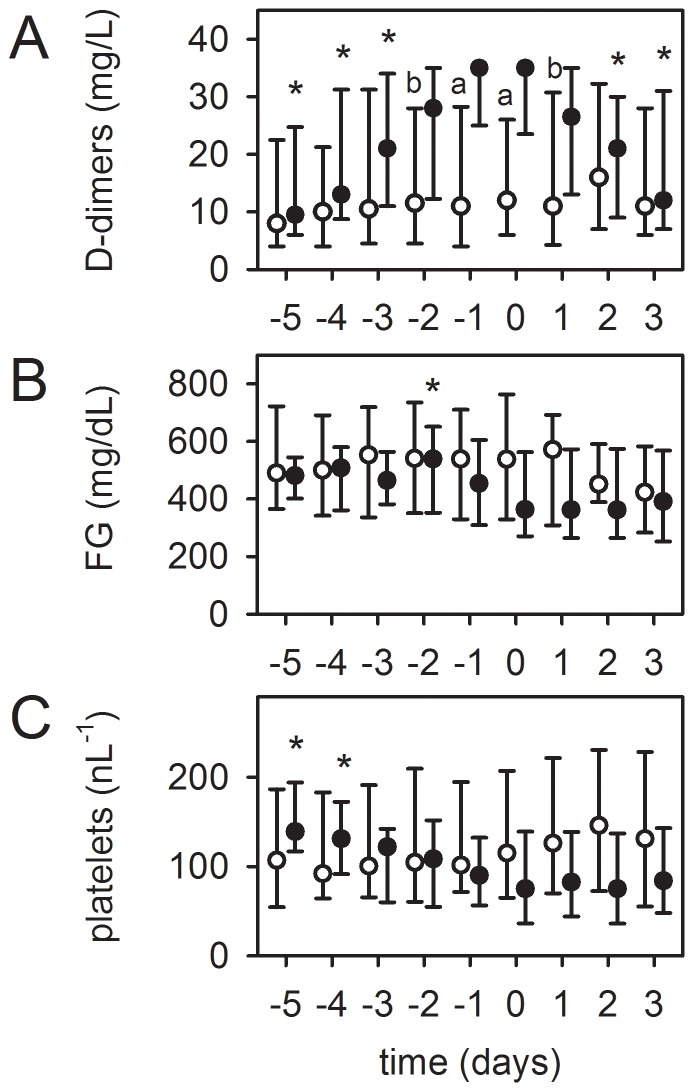
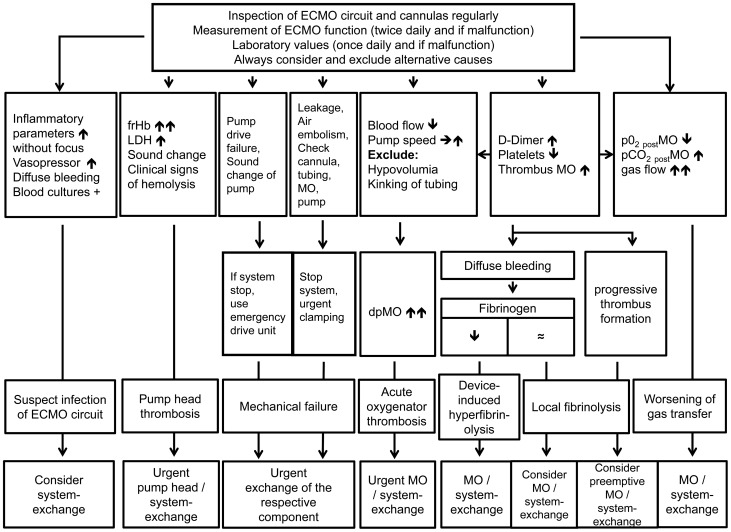
Results: Values presented as median (interquartile range). Patient age was 50(36-60) years, the SOFA score 11(8-14.3) and the Murray lung injury Score 3.33(3.3-3.7). Cumulative ECMO support time 3411 days, 9(6-15) days per patient. Mechanical failure of the blood pump (n = 5), MO (n = 2) or cannula (n = 1) accounted for 10% of the exchanges. Acute clot formation within the pump head (visible clots, increase in plasma free hemoglobin (frHb), serum lactate dehydrogenase (LDH), n = 13) and MO (increase in pressure drop across the MO, n = 16) required an urgent system-exchange, of which nearly 50% could be foreseen by measuring the parameters mentioned below. Reasons for an elective system-exchange were worsening of gas transfer capability (n = 10) and device-related coagulation disorders (n = 32), either local fibrinolysis in the MO due to clot formation (increased D-dimers [DD]), decreased platelet count; n = 24), or device-induced hyperfibrinolysis (increased DD, decreased fibrinogen [FG], decreased platelet count, diffuse bleeding tendency; n = 8), which could be reversed after system-exchange. Four MOs were exchanged due to suspicion of infection.
Conclusions: The majority of ECMO system-exchanges could be predicted by regular inspection of the complete ECMO circuit, evaluation of gas exchange, pressure drop across the MO and laboratory parameters (DD, FG, platelets, LDH, frHb). These parameters should be monitored in the daily routine to reduce the risk of unexpected ECMO failure.
Conflict of interest statement
Figures
References
-
- MacLaren G, Combes A, Bartlett RH (2012) Contemporary extracorporeal membrane oxygenation for adult respiratory failure: life support in the new era. Intensive Care Med 38:210–220. - PubMed
-
- Peek GJ, Elbourne D, Mugford M, Tiruvoipati R, Wilson A, et al. (2010) Randomised controlled trial and parallel economic evaluation of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR). Health Technol Assess 14:1–46. - PubMed
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, et al. (2009) Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 374:1351–1363. - PubMed
-
- Australia, New Zealand Extracorporeal Membrane Oxygenation Influenza I Davies A, Jones D, Bailey M, et al. (2009) Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA 302:1888–1895. - PubMed
-
- Combes A, Pellegrino V (2011) Extracorporeal membrane oxygenation for 2009 influenza A (H1N1)-associated acute respiratory distress syndrome. Semin Respir Crit Care Med 32:188–194. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
