

Extended duration dual antiplatelet therapy and mortality: a systematic review and meta-analysis
- PMID: 25467565
- PMCID: PMC4386690
- DOI: 10.1016/S0140-6736(14)62052-3
Extended duration dual antiplatelet therapy and mortality: a systematic review and meta-analysis
Erratum in
-
Department of Error.Lancet. 2015 May 9;385(9980):1834. doi: 10.1016/S0140-6736(15)60927-8. Lancet. 2015. PMID: 25987156 No abstract available.
Abstract
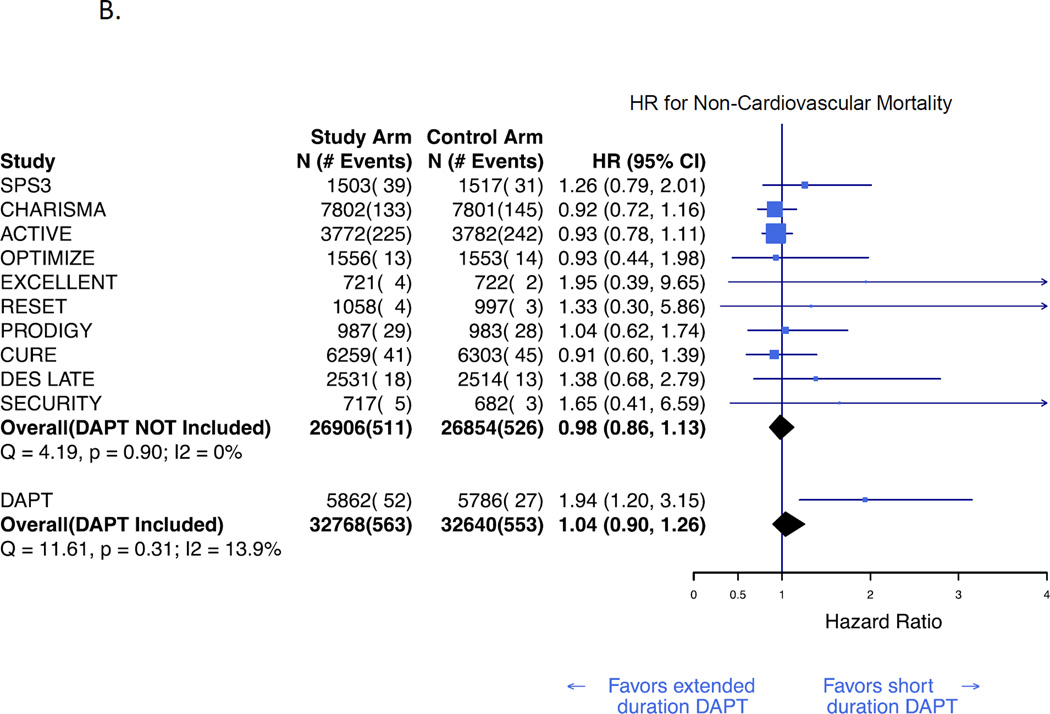
Background: Treatment with aspirin and a P2Y12 inhibitor is commonly used in patients with cardiovascular disorders. The overall effect of such treatment on all-cause mortality is unknown. In the Dual Antiplatelet Therapy (DAPT) Study, continuation of dual antiplatelet therapy beyond 12 months after coronary stenting was associated with an unexpected increase in non-cardiovascular death. In view of the potential public health importance of these findings, we aimed to assess the effect of extended duration dual antiplatelet therapy on mortality by doing a meta-analysis of all randomised, controlled trials of treatment duration in various cardiovascular disorders.
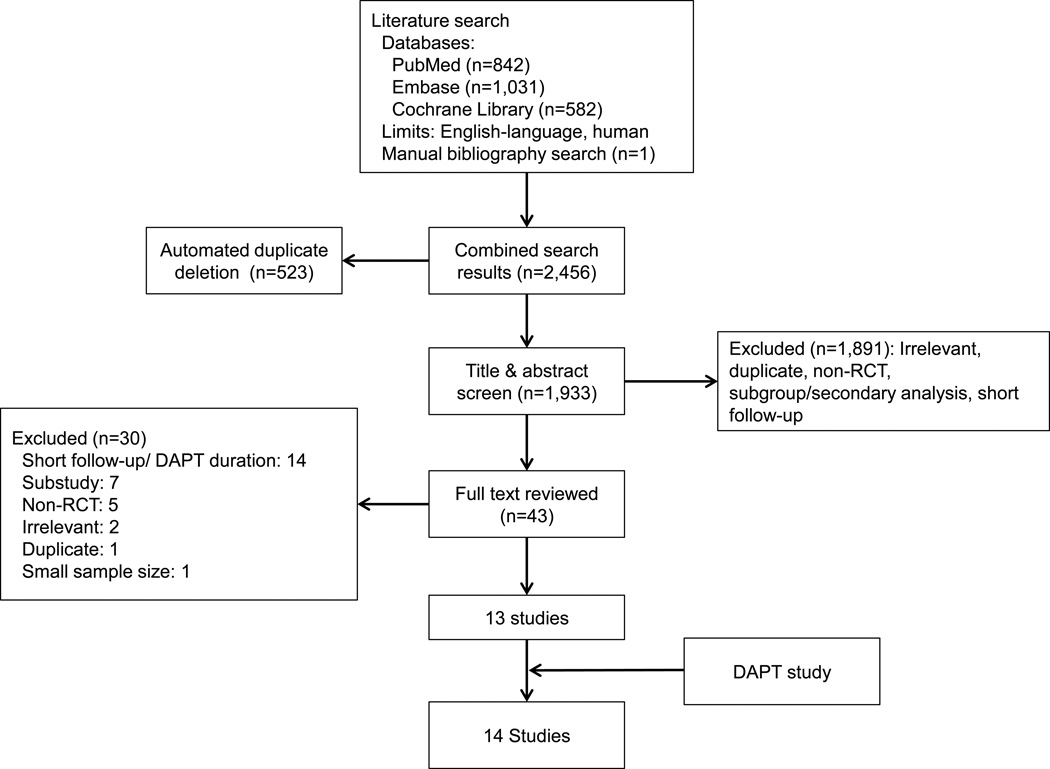
Methods: We searched Medline, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) to identify randomised controlled trials assessing the effect of extended duration versus no or short duration dual antiplatelet therapy, published before Oct 1, 2014. We did a meta-analysis to pool results with a hierarchical Bayesian random-effects model. The primary outcomes were hazard ratios comparing rates of all-cause, cardiovascular, and non-cardiovascular death.
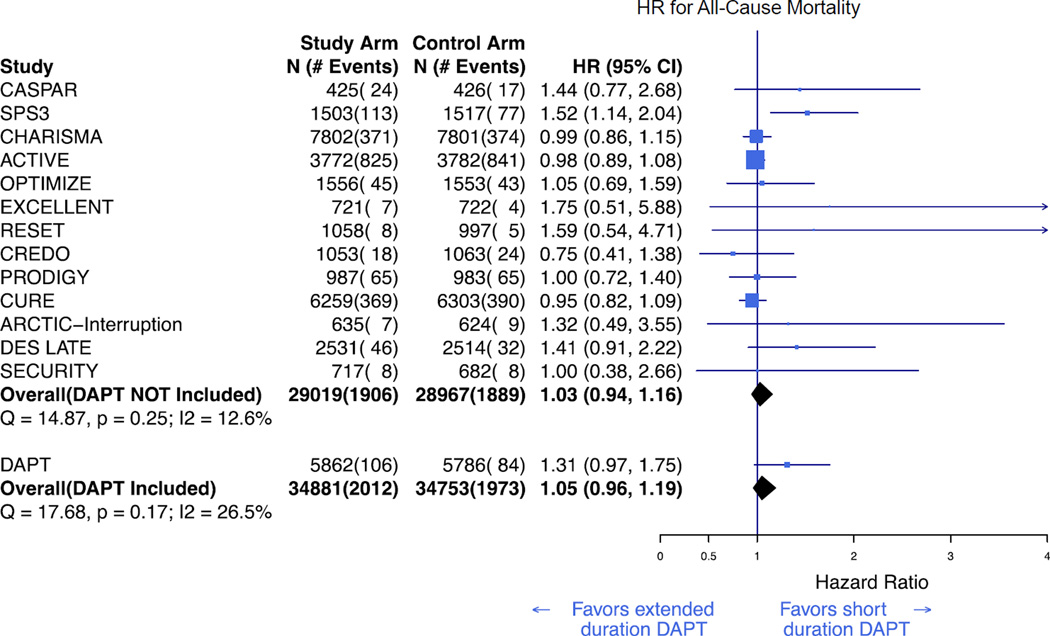
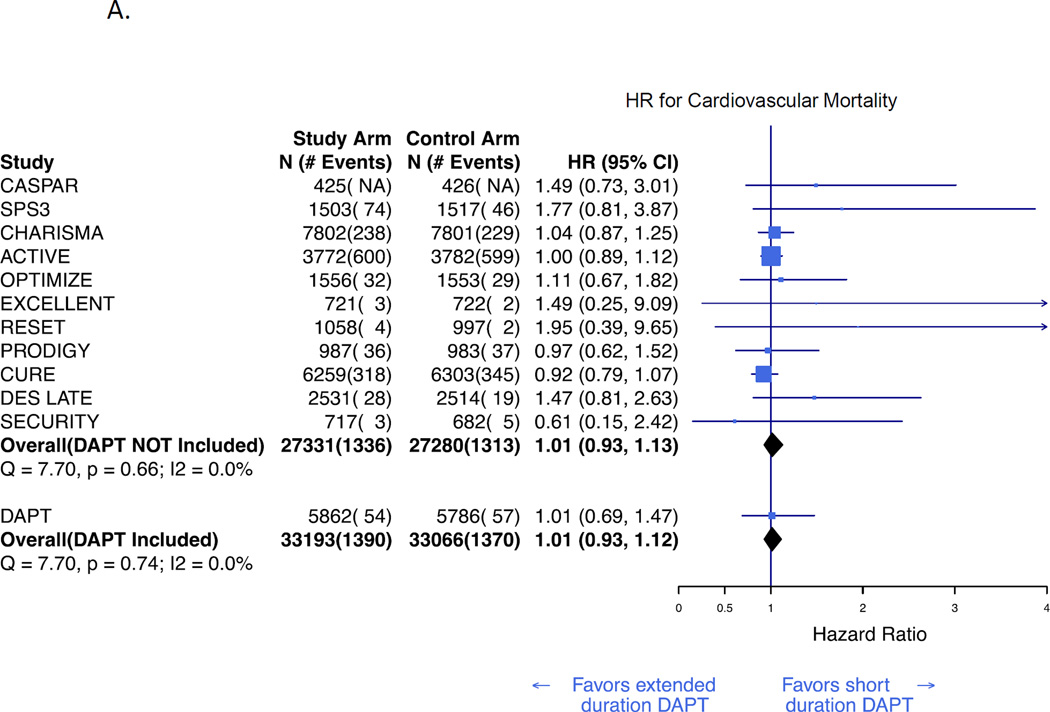
Findings: Including the DAPT Study, we identified 14 eligible trials that randomly assigned 69,644 participants to different durations of dual antiplatelet therapy. Compared with aspirin alone or short duration dual antiplatelet therapy (≤6 months), continued treatment was not associated with a difference in all-cause mortality (hazard ratio [HR] 1·05, 95% credible interval [CrI] 0·96-1·19; p=0·33). Similarly, cardiovascular (1·01, 0·93-1·12; p=0·81) and non-cardiovascular mortality (1·04, 0·90-1·26; p=0·66) were no different with extended duration versus short duration dual antiplatelet therapy or aspirin alone.
Interpretation: Extended duration dual antiplatelet therapy was not associated with a difference in the risk of all-cause, cardiovascular, or non-cardiovascular death compared with aspirin alone or short duration dual antiplatelet therapy.
Funding: None.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Antiplatelet therapy: risks and benefits of extended DAPT after stenting.Nat Rev Cardiol. 2015 Jan;12(1):1. doi: 10.1038/nrcardio.2014.192. Epub 2014 Dec 2. Nat Rev Cardiol. 2015. PMID: 25445134 No abstract available.
-
Dual antiplatelet therapy and non-cardiovascular mortality.Lancet. 2015 Feb 28;385(9970):756-7. doi: 10.1016/S0140-6736(14)62125-5. Epub 2014 Nov 16. Lancet. 2015. PMID: 25467568 No abstract available.
-
Dual antiplatelet therapy duration and mortality - Authors' reply.Lancet. 2015 May 30;385(9983):2149-50. doi: 10.1016/S0140-6736(15)61019-4. Lancet. 2015. PMID: 26068262 No abstract available.
-
Dual antiplatelet therapy duration and mortality.Lancet. 2015 May 30;385(9983):2149. doi: 10.1016/S0140-6736(15)61018-2. Lancet. 2015. PMID: 26068263 No abstract available.
References
-
- Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. The New England journal of medicine. 2006;354(16):1706–1717. - PubMed
-
- Mauri L, Kereiakes DJ, Yeh RW, et al. Continuation of dual antiplatelet therapy beyond one year after drug-eluting coronary stent procedures. New England journal of medicine. 2014
-
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Annals of internal medicine. 2009;151(4):W65–W94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
