

Increase in anaphylaxis-related hospitalizations but no increase in fatalities: an analysis of United Kingdom national anaphylaxis data, 1992-2012
- PMID: 25468198
- PMCID: PMC4382330
- DOI: 10.1016/j.jaci.2014.10.021
Increase in anaphylaxis-related hospitalizations but no increase in fatalities: an analysis of United Kingdom national anaphylaxis data, 1992-2012
Abstract
Background: The incidence of anaphylaxis might be increasing. Data for fatal anaphylaxis are limited because of the rarity of this outcome.
Objective: We sought to document trends in anaphylaxis admissions and fatalities by age, sex, and cause in England and Wales over a 20-year period.
Methods: We extracted data from national databases that record hospital admissions and fatalities caused by anaphylaxis in England and Wales (1992-2012) and crosschecked fatalities against a prospective fatal anaphylaxis registry. We examined time trends and age distribution for fatal anaphylaxis caused by food, drugs, and insect stings.
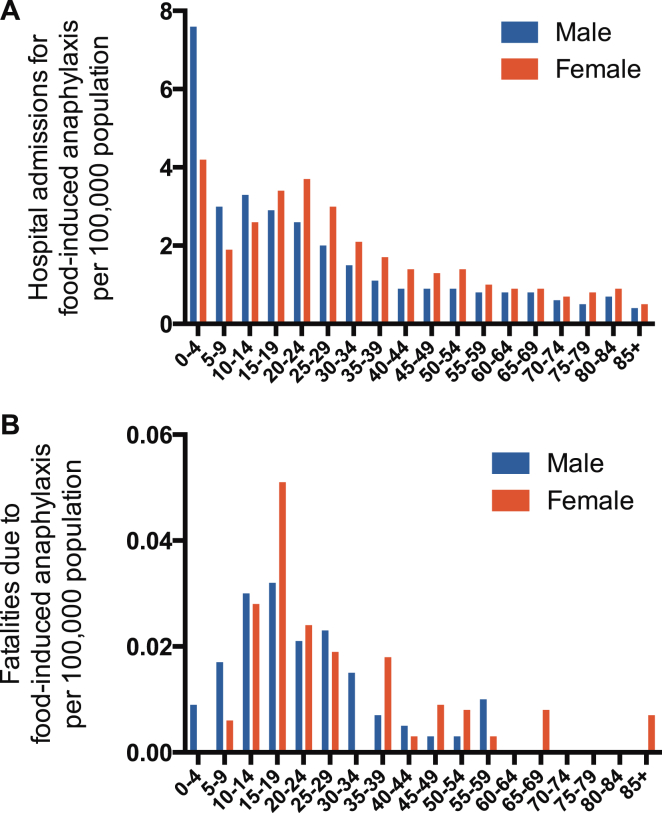
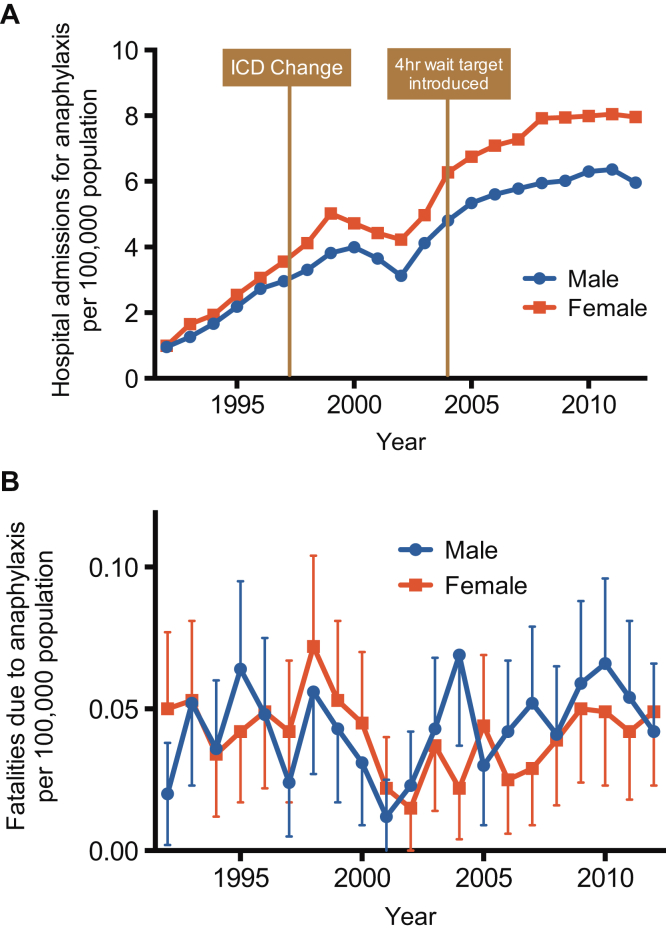
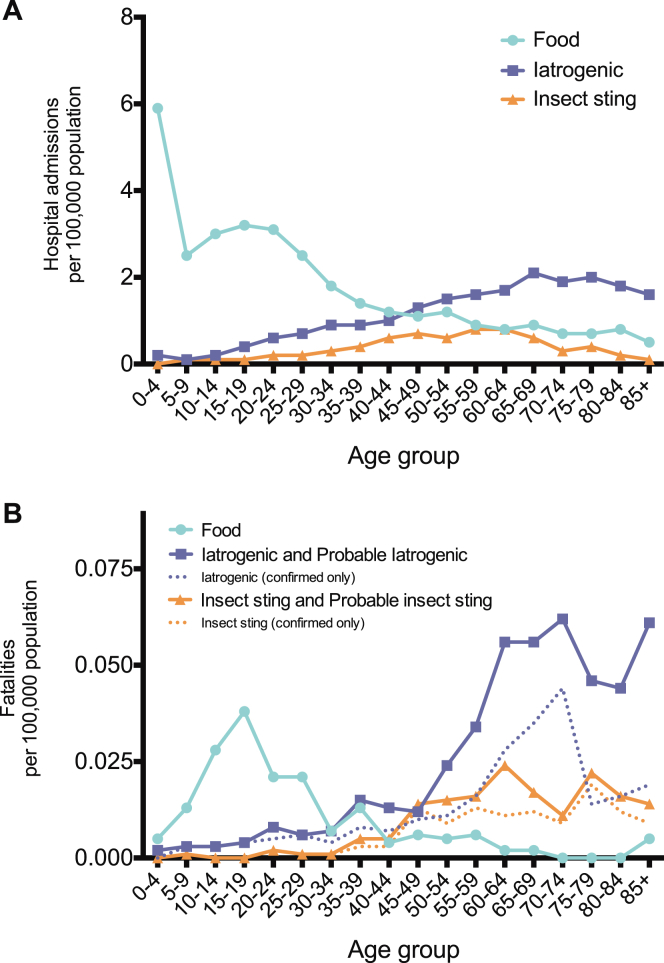
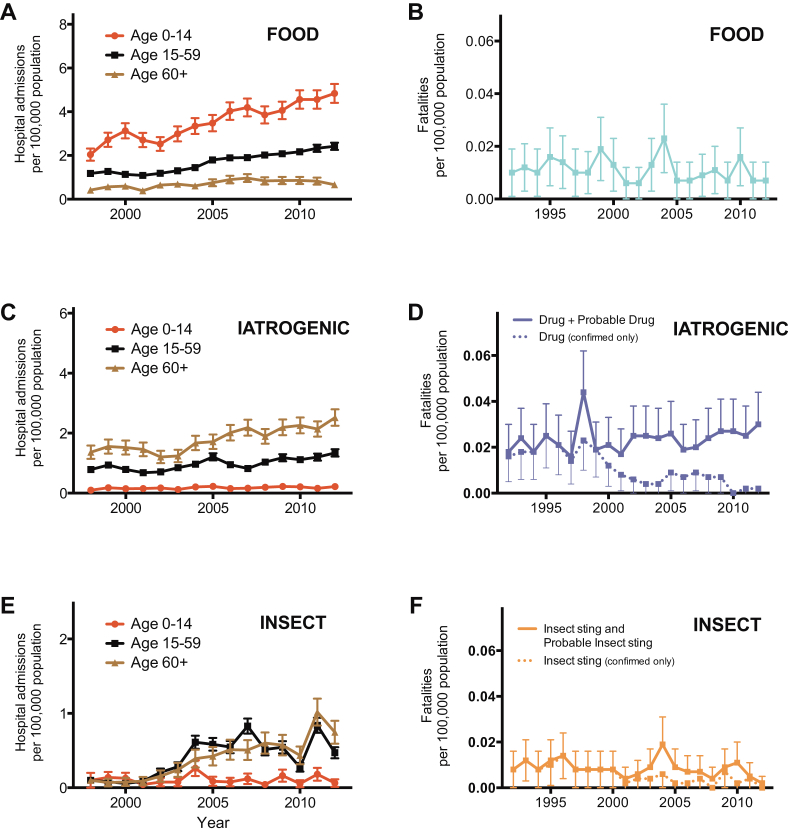
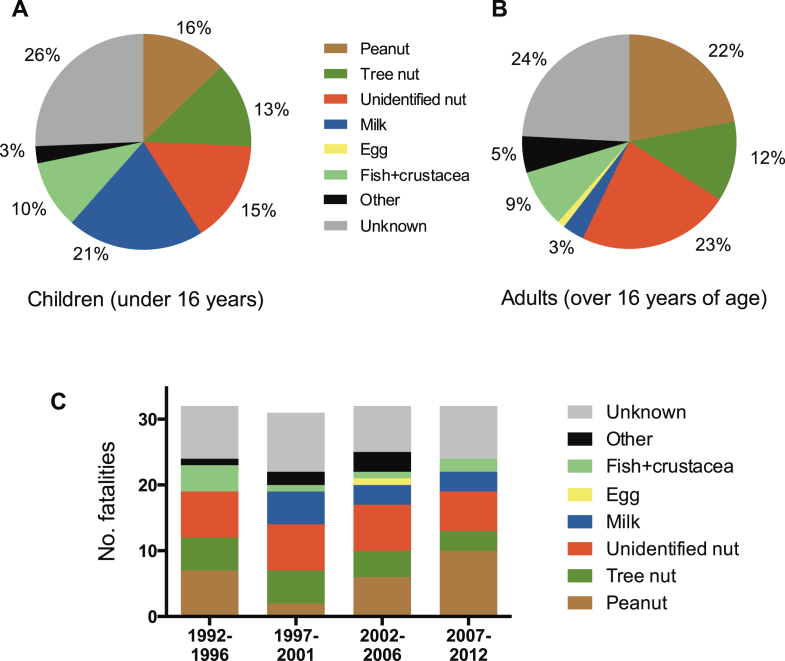
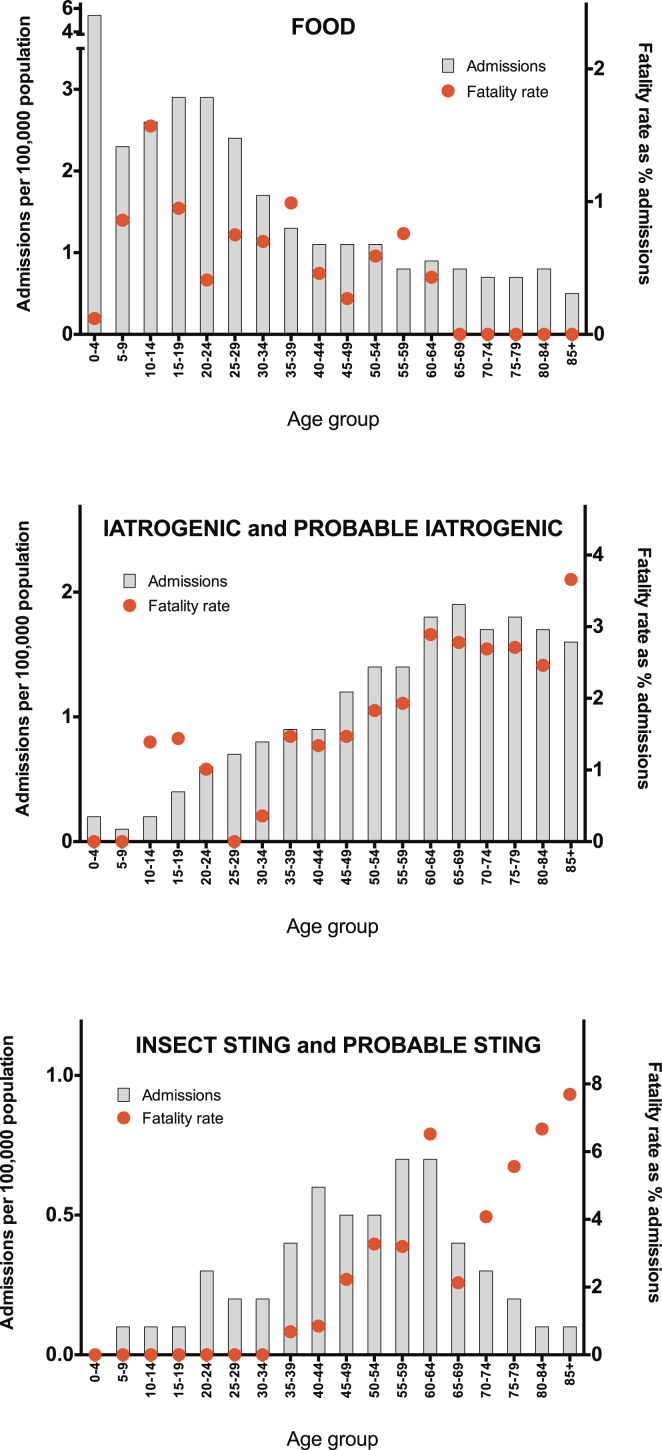
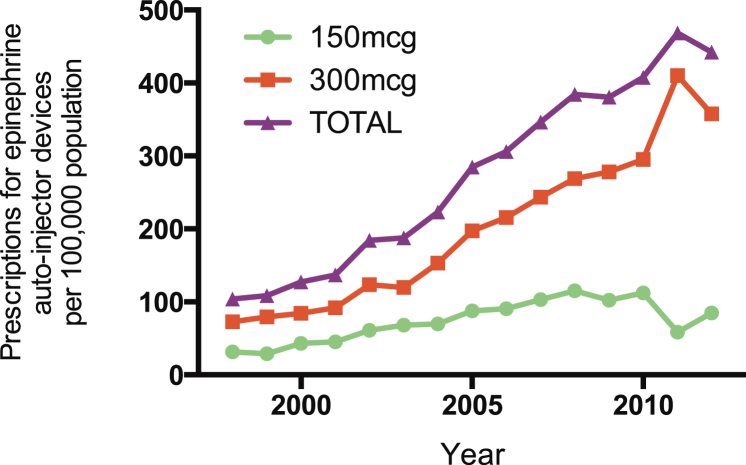
Results: Hospital admissions from all-cause anaphylaxis increased by 615% over the time period studied, but annual fatality rates remained stable at 0.047 cases (95% CI, 0.042-0.052 cases) per 100,000 population. Admission and fatality rates for drug- and insect sting-induced anaphylaxis were highest in the group aged 60 years and older. In contrast, admissions because of food-triggered anaphylaxis were most common in young people, with a marked peak in the incidence of fatal food reactions during the second and third decades of life. These findings are not explained by age-related differences in rates of hospitalization.
Conclusions: Hospitalizations for anaphylaxis increased between 1992 and 2012, but the incidence of fatal anaphylaxis did not. This might be due to increasing awareness of the diagnosis, shifting patterns of behavior in patients and health care providers, or both. The age distribution of fatal anaphylaxis varies significantly according to the nature of the eliciting agent, which suggests a specific vulnerability to severe outcomes from food-induced allergic reactions in the second and third decades.
Keywords: Anaphylaxis; drug allergy; epidemiology; food allergy; hospitalization; insect sting allergy.
Copyright © 2014 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Pumphrey R.S. Lessons for management of anaphylaxis from a study of fatal reactions. Clin Exp Allergy. 2000;30:1144–1150. - PubMed
-
- Cummings A.J., Knibb R.C., King R.M., Lucas J.S. The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their families: a review. Allergy. 2010;65:933–945. - PubMed
-
- Lau G.Y., Patel N., Umasunthar T., Gore C., Warner J.O., Hanna H. Anxiety and stress in mothers of food-allergic children. Pediatr Allergy Immunol. 2014;25:236–242. - PubMed
-
- Poulos L.M., Waters A.M., Correll P.K., Loblay R.H., Marks G.B. Trends in hospitalizations for anaphylaxis, angioedema, and urticaria in Australia, 1993-1994 to 2004-2005. J Allergy Clin Immunol. 2007;120:878–884. - PubMed
-
- Wood R.A., Camargo C.A., Jr., Lieberman P., Sampson H.A., Schwartz L.B., Zitt M. Anaphylaxis in America: the prevalence and characteristics of anaphylaxis in the United States. J Allergy Clin Immunol. 2014;133:461–467. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
