

Radiofrequency ablation to treat loco-regional recurrence of well-differentiated thyroid carcinoma
- PMID: 25469095
- PMCID: PMC4248639
- DOI: 10.3348/kjr.2014.15.6.817
Radiofrequency ablation to treat loco-regional recurrence of well-differentiated thyroid carcinoma
Abstract
Objective: To evaluate the efficacy of radiofrequency ablation (RFA) in the treatment of loco-regional, recurrent, and well-differentiated thyroid carcinoma.
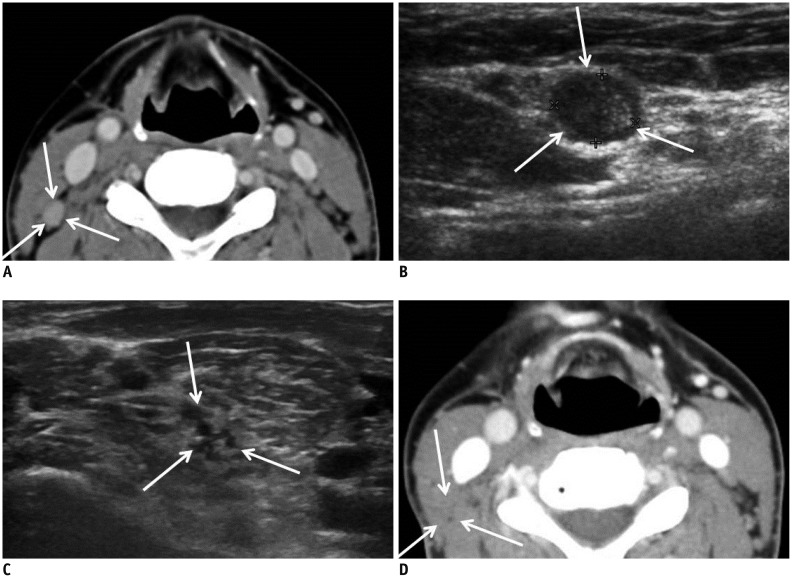
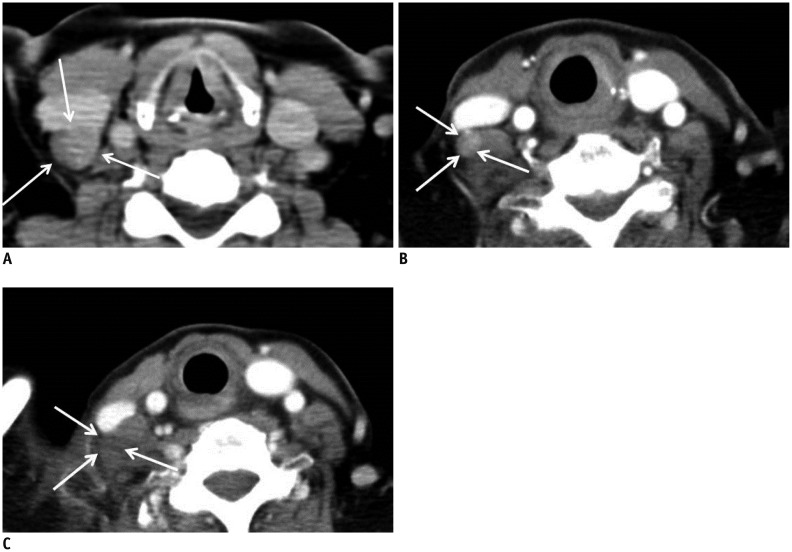
Materials and methods: Thirty-five recurrent well-differentiated thyroid carcinomas (RTC) in 32 patients were treated with RFA, between March 2008 and October 2011. RTCs were detected by regular follow-up ultrasound and confirmed by biopsy. All patients had fewer than 3 RTCs in the neck and were at high surgical risk or refused to undergo repeated surgery. Average number of RFA sessions were 1.3 (range 1-3). Post-RFA biopsy and ultrasound were performed. The mean follow-up period was 30 months. Pre- and post-RFA serum thyroglobulin values were evaluated.
Results: Thirty-one patients with 33 RTCs were treated with RFA only, whereas 1 patient with 2 RTCs was treated with RFA followed by surgery. At the last follow-up ultrasound, 31 (94%) of the 33 RTCs treated with RFA alone completely disappeared and the remaining 2 (6%) RTCs showed decreased volume. The largest diameter and volume of the 33 RTCs were markedly decreased by 93.2% (from 8.1 ± 3.4 mm to 0.6 ± 1.8 mm, p < 0.001) and 96.4% (from 173.9 ± 198.7 mm(3) to 6.2 ± 27.9 mm(3), p < 0.001), respectively. Twenty of the 21 RTCs evaluated with post-RFA biopsies (95%) were negative for malignancy. One (5%) showed remaining tumor that was removed surgically. The serum thyroglobulin was decreased in 19 of 26 patients (73%). Voice change developed immediately after RFA in 6 patients (19%) and was spontaneously recovered in 5 patients (83%).
Conclusion: Radiofrequency ablation can be effective in treating loco-regional, recurrent, and well-differentiated thyroid carcinoma in patients at high surgical risk.
Keywords: Efficacy; Radiofrequency ablation; Recurrent thyroid cancer; Thyroid; Ultrasound.
Figures



References
-
- Kumar V, Abbas AK, Aster JC. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Philadelphia: Saunders; 2014. pp. 1073–1139.
-
- Gilliland FD, Hunt WC, Morris DM, Key CR. Prognostic factors for thyroid carcinoma. A population-based study of 15,698 cases from the Surveillance, Epidemiology and End Results (SEER) program 1973-1991. Cancer. 1997;79:564–573. - PubMed
-
- Dupuy DE, Monchik JM. Radiofrequency ablation of recurrent thyroid cancer. In: Ellis LM, Curley SA, Tanabe KK, editors. Radiofrequency Ablation for Cancer: Current indications, techniques, and outcomes. New York: Springer-Verlag; 2003. pp. 213–223.
-
- Loh KC, Greenspan FS, Gee L, Miller TR, Yeo PP. Pathological tumor-node-metastasis (pTNM) staging for papillary and follicular thyroid carcinomas: a retrospective analysis of 700 patients. J Clin Endocrinol Metab. 1997;82:3553–3562. - PubMed
-
- Samaan NA, Schultz PN, Hickey RC, Goepfert H, Haynie TP, Johnston DA, et al. The results of various modalities of treatment of well differentiated thyroid carcinomas: a retrospective review of 1599 patients. J Clin Endocrinol Metab. 1992;75:714–720. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
