

Moving-shot versus fixed electrode techniques for radiofrequency ablation: comparison in an ex-vivo bovine liver tissue model
- PMID: 25469097
- PMCID: PMC4248641
- DOI: 10.3348/kjr.2014.15.6.836
Moving-shot versus fixed electrode techniques for radiofrequency ablation: comparison in an ex-vivo bovine liver tissue model
Abstract
Objective: To compare the ablation characteristics of the moving-shot technique (MST) and the fixed electrode technique (FET) for radiofrequency (RF) ablation in an ex-vivo bovine liver tissue model.
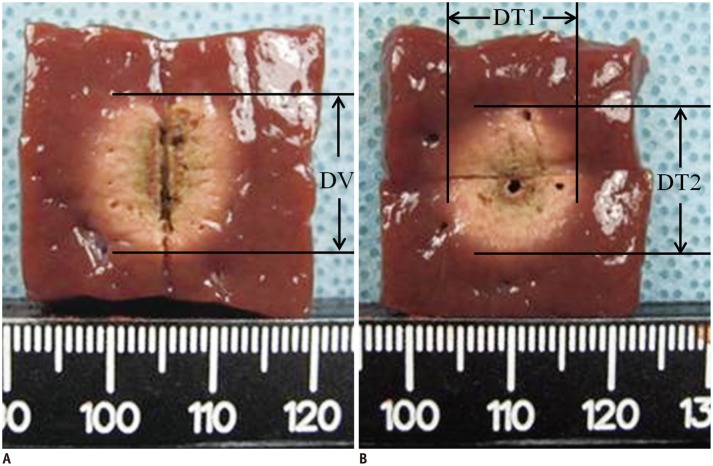
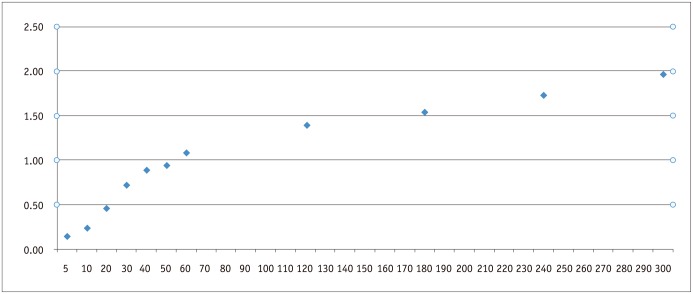
Materials and methods: We performed RF ablation using FET in 110 bovine liver blocks using 11 different ablation times ranging from 5 seconds to 5 minutes (10 blocks per each time duration). Ten bovine liver blocks at each ablation time of 1- or 2-minute, were ablated with MST, which treated conceptual ablation units by moving the electrode tip. We evaluated the ablation volume obtained with FET across ablation time lengths. The results of FET and MST performed with the same ablation time lengths, i.e., 1- and 2-minute ablation time were also compared.
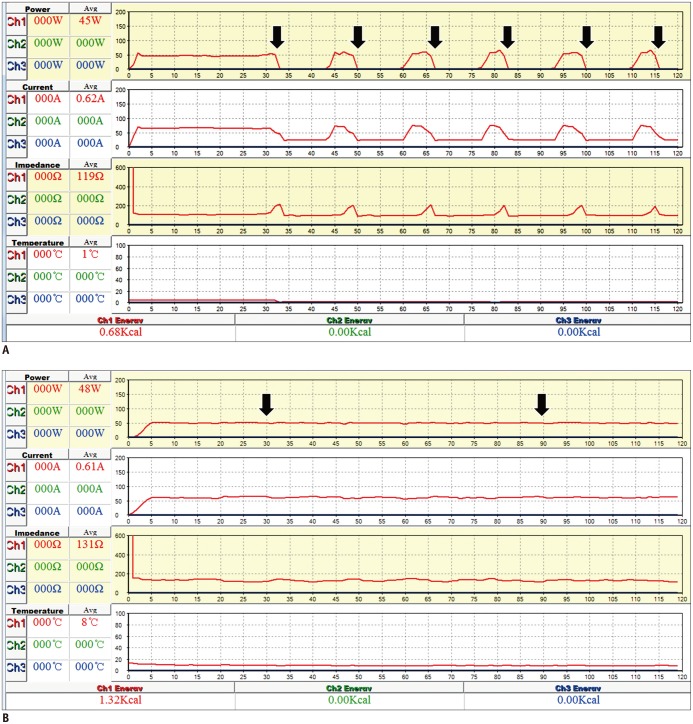
Results: The ablation volume achieved with FET gradually increased with increasing ablation time; however, the pair-wise statistical comparison between 2 neighboring ablation time lengths was not significant after 30 seconds. MST with either 1- or 2-minute ablation time achieved larger ablation volumes (1.1 ± 0.2 mL vs. 2.7 ± 0.3 mL, p < 0.001; and 1.4 ± 0.2 mL vs. 5.6 ± 0.4 mL, p < 0.001, respectively), longer true RF times (46.7 ± 4.6 seconds vs. 60 seconds, p < 0.001; and 64.8 ± 4.6 seconds vs. 120 seconds, p < 0.001, respectively), fewer numbers of RF cut-offs (1.6 ± 0.5 vs. 0, p < 0.001; and 5.5 ± 0.5 vs. 0, p < 0.001, respectively), and greater energy deposition (2050.16 ± 209.2 J vs. 2677.76 ± 83.68 J, p < 0.001; and 2970.64 ± 376.56 J vs. 5564.72 ± 5439.2 J, p < 0.001, respectively), than FET.
Conclusion: The MST can achieve a larger ablation volume by preventing RF cut-off, compared with the FET in an ex-vivo bovine liver model.
Keywords: Fixed electrode technique; Intervention; Moving shot technique; Radiofrequency ablation; Thyroid nodule.
Figures
References
-
- Dupuy DE, Zagoria RJ, Akerley W, Mayo-Smith WW, Kavanagh PV, Safran H. Percutaneous radiofrequency ablation of malignancies in the lung. AJR Am J Roentgenol. 2000;174:57–59. - PubMed
-
- Dupuy DE, Goldberg SN. Image-guided radiofrequency tumor ablation: challenges and opportunities--part II. J Vasc Interv Radiol. 2001;12:1135–1148. - PubMed
-
- Gazelle GS, Goldberg SN, Solbiati L, Livraghi T. Tumor ablation with radio-frequency energy. Radiology. 2000;217:633–646. - PubMed
-
- Goldberg SN. Radiofrequency tumor ablation: principles and techniques. Eur J Ultrasound. 2001;13:129–147. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
