

The Chicago Classification of esophageal motility disorders, v3.0
- PMID: 25469569
- PMCID: PMC4308501
- DOI: 10.1111/nmo.12477
The Chicago Classification of esophageal motility disorders, v3.0
Abstract
Background: The Chicago Classification (CC) of esophageal motility disorders, utilizing an algorithmic scheme to analyze clinical high-resolution manometry (HRM) studies, has gained acceptance worldwide.
Methods: This 2014 update, CC v3.0, developed by the International HRM Working Group, incorporated the extensive clinical experience and interval publications since the prior (2011) version.
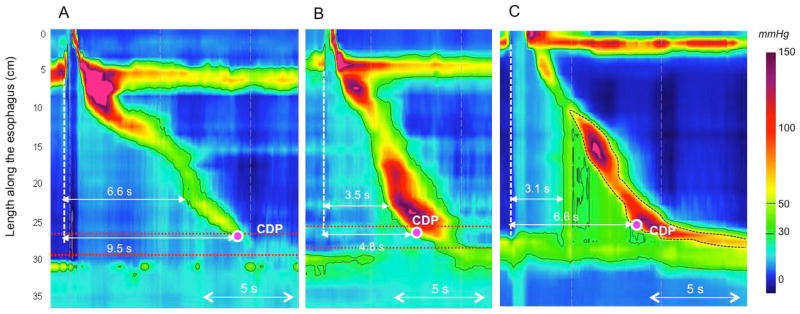
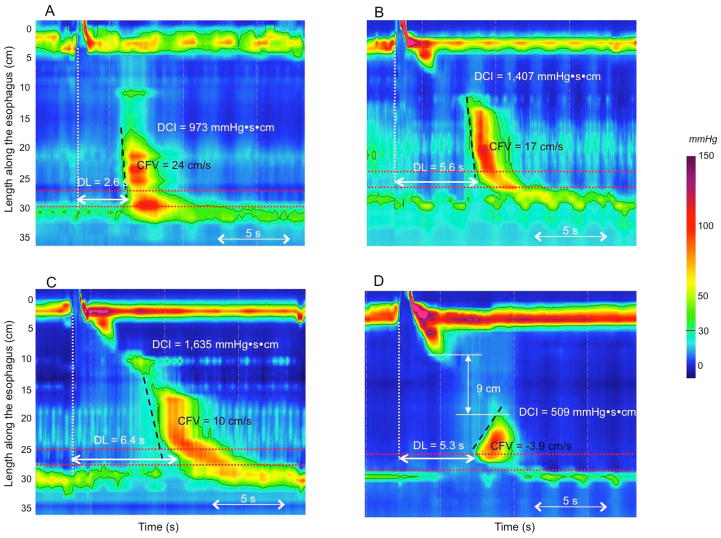
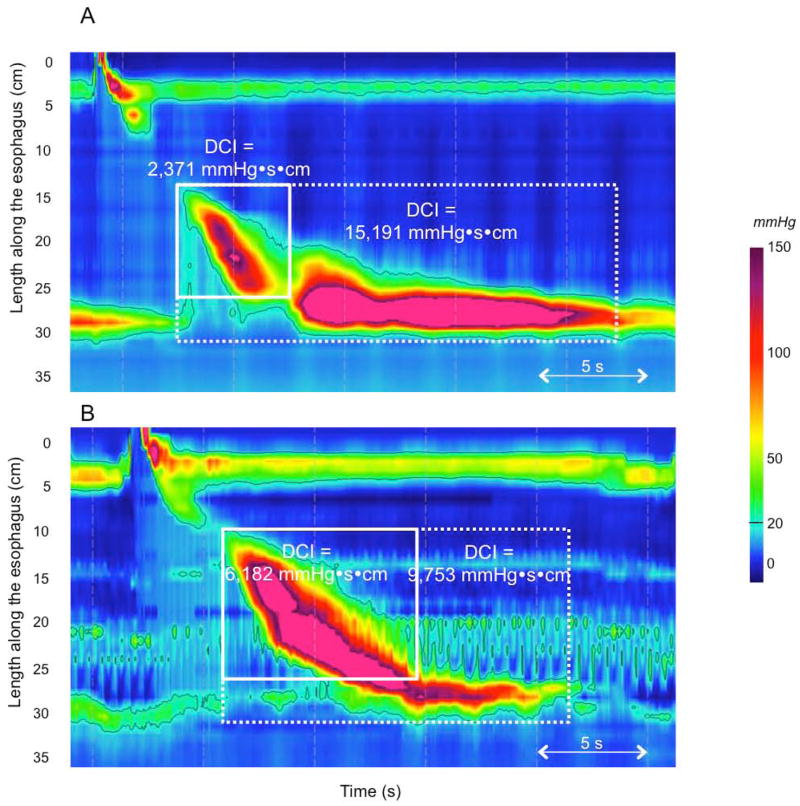
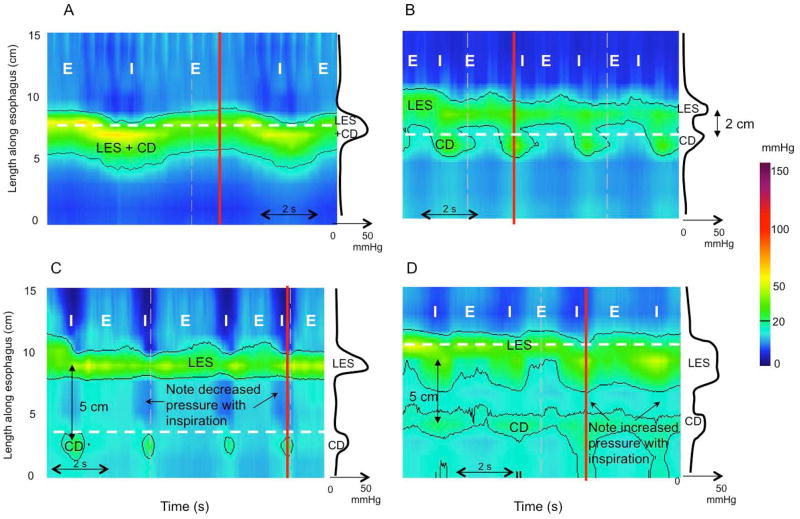
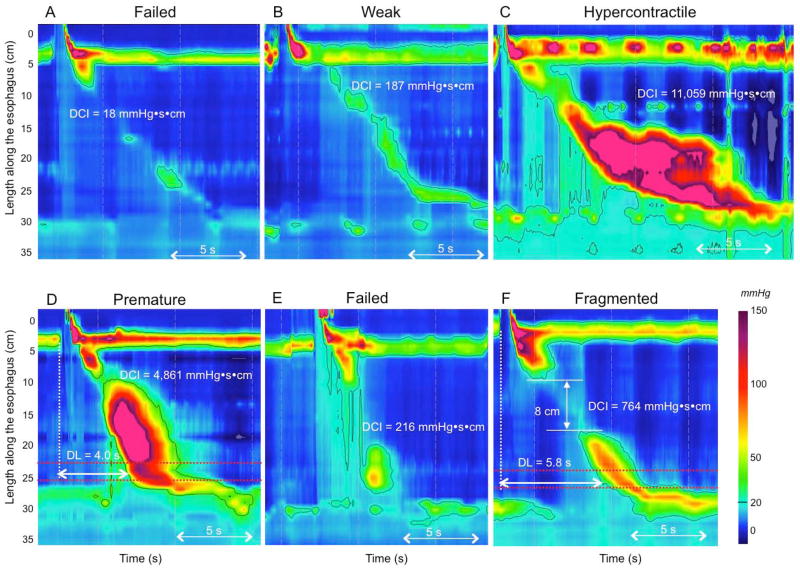
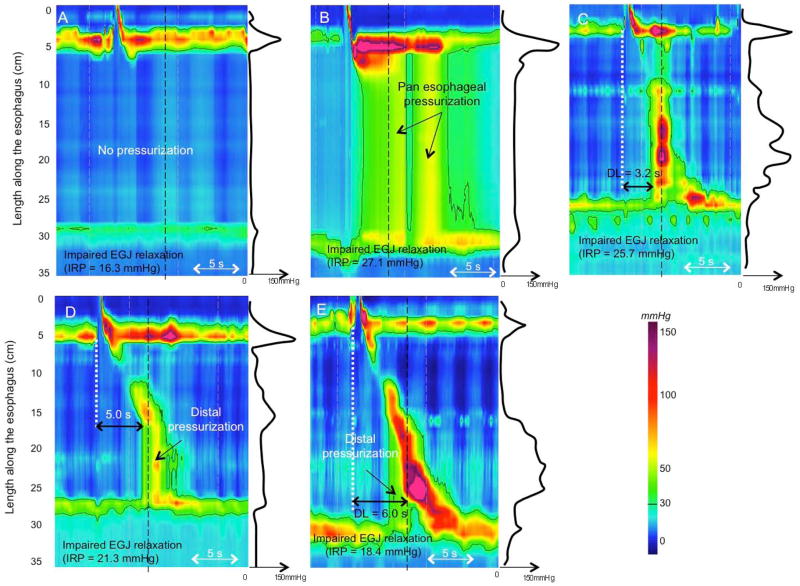
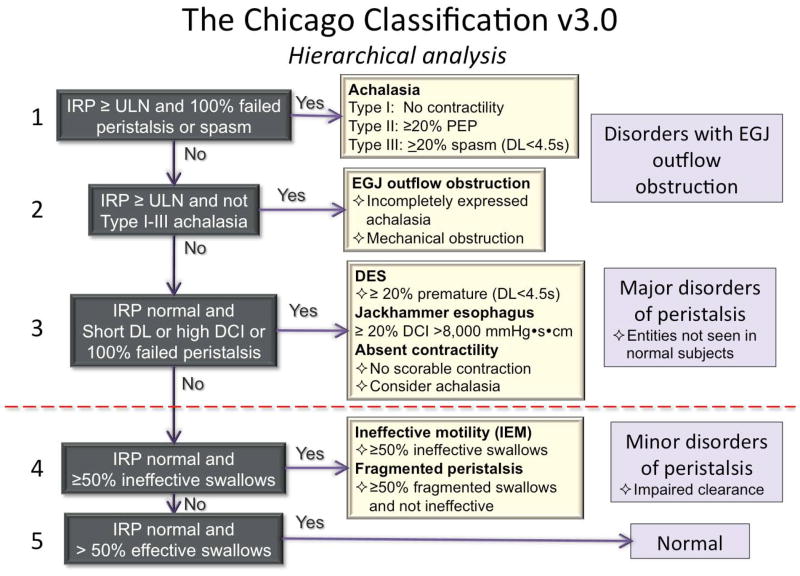
Key results: Chicago Classification v3.0 utilizes a hierarchical approach, sequentially prioritizing: (i) disorders of esophagogastric junction (EGJ) outflow (achalasia subtypes I-III and EGJ outflow obstruction), (ii) major disorders of peristalsis (absent contractility, distal esophageal spasm, hypercontractile esophagus), and (iii) minor disorders of peristalsis characterized by impaired bolus transit. EGJ morphology, characterized by the degree of overlap between the lower esophageal sphincter and the crural diaphragm and baseline EGJ contractility are also part of CC v3.0. Compared to the previous CC version, the key metrics of interpretation, the integrated relaxation pressure (IRP), the distal contractile integral (DCI), and the distal latency (DL) remain unchanged, albeit with much more emphasis on DCI for defining both hypo- and hypercontractility. New in CC v3.0 are: (i) the evaluation of the EGJ at rest defined in terms of morphology and contractility, (ii) 'fragmented' contractions (large breaks in the 20-mmHg isobaric contour), (iii) ineffective esophageal motility (IEM), and (iv) several minor adjustments in nomenclature and defining criteria. Absent in CC v3.0 are contractile front velocity and small breaks in the 20-mmHg isobaric contour as defining characteristics.
Conclusions & inferences: Chicago Classification v3.0 is an updated analysis scheme for clinical esophageal HRM recordings developed by the International HRM Working Group.
Keywords: achalasia; dysphagia; esophageal motility disorders; high-resolution manometry; ineffective esophageal motility.
© 2014 John Wiley & Sons Ltd.
Conflict of interest statement
COMPETING INTERESTS
Albert J Bredenoord: Given Imaging: research funding; Medical Measurement Systems: educational and research funding
Mark Fox: Given imaging: advisory board, consulting and educational; Sandhill Scientific: educational; Medical Measurement Systems: educational.
C Prakash Gyawali: Given imaging, educational
John E Pandolfino: Given imaging; consulting and educational
Serhat Bor: Medical Measurement Systems: educational and research funding
DO Castell: Sandhill Scientific Instruments; consultant and educational
Jeffrey L Conklin: Given imaging: consulting and educational
Sabine Roman: Given imaging: advisory board, consulting and educational
Phil Katz: Torax: consultant; Prizer Consumer: consultant
Jutta Keller: Given imaging: research funding, consulting and educational; Standard Imaging: consulting and educational
Taher Omari: Sandhill Scientific Instruments: consulting and research grant; Medical Measurement Systems: educational.
Edoardo Savarino: Given imaging; advisory board, consulting and educational
Felice Schnoll-Sussman: Given imaging; advisory board, consulting and educational
Daniel Sifrim: Given imaging; advisory board. Sandhill Scientific Instruments: research grant.
Rami Sweis: Given imaging; consulting and educational
Radu Tutuian: Sandhill Scientific Instruments: educational; Medical Measurement Systems: educational.
Marcelo F Vela: Given Imaging, Consulting
Frank Zerbib: Given imaging; advisory board, consulting, and educational.
Figures
References
-
- Gyawali CP. High resolution manometry: the Ray Clouse legacy. Neurogastroenterol Motil. 2012 Mar 24;(Suppl 1):2–4. - PubMed
-
- Bogte A, Bredenoord AJ, Oors J, Siersema PD, Smout AJ. Normal values for esophageal high-resolution manometry. Neurogastroenterol Motil. 2013;25:762–e579. - PubMed
-
- Shi Y, Xiao Y, Peng S, Lin J, Xiong L, Chen M. Normative data of high-resolution impedance manometry in the Chinese population. J Gastroenterol Hepatol. 2013;28:1611–1615. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
