

Organizational predictors of colonoscopy follow-up for positive fecal occult blood test results: an observational study
- PMID: 25471345
- PMCID: PMC4323731
- DOI: 10.1158/1055-9965.EPI-14-1170
Organizational predictors of colonoscopy follow-up for positive fecal occult blood test results: an observational study
Abstract
Background: This study assessed the contribution of organizational structures and processes identified from facility surveys to follow-up for positive fecal occult blood tests [FOBT-positive (FOBT(+))].
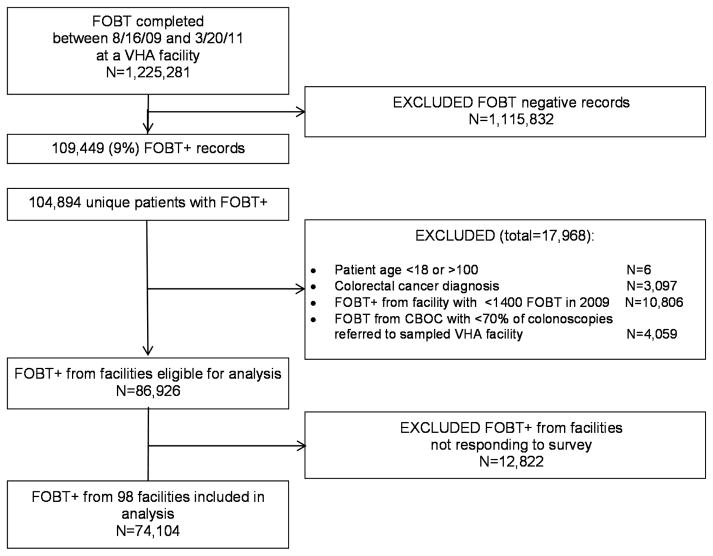
Methods: We identified 74,104 patients with FOBT(+) results from 98 Veterans Health Administration (VHA) facilities between August 16, 2009 and March 20, 2011, and followed them until September 30, 2011, for completion of colonoscopy. We identified patient characteristics from VHA administrative records, and organizational factors from facility surveys completed by primary care and gastroenterology chiefs. We estimated predictors of colonoscopy completion within 60 days and six months using hierarchical logistic regression models.
Results: Thirty percent of patients with FOBT(+) results received colonoscopy within 60 days and 49% within six months. Having gastroenterology or laboratory staff notify gastroenterology providers directly about FOBT(+) cases was a significant predictor of 60-day [odds ratio (OR), 1.85; P = 0.01] and six-month follow-up (OR, 1.25; P = 0.008). Additional predictors of 60-day follow-up included adequacy of colonoscopy appointment availability (OR, 1.43; P = 0.01) and frequent individual feedback to primary care providers about FOBT(+) referral timeliness (OR, 1.79; P = 0.04). Additional predictors of six-month follow-up included using guideline-concordant surveillance intervals for low-risk adenomas (OR, 1.57; P = 0.01) and using group appointments and combined verbal-written methods for colonoscopy preparation instruction (OR, 1.48; P = 0.0001).
Conclusion: Directly notifying gastroenterology providers about FOBT(+) results, using guideline-concordant adenoma surveillance intervals, and using colonoscopy preparations instruction methods that provide both verbal and written information may increase overall follow-up rates. Enhancing follow-up within 60 days may require increased colonoscopy capacity and feedback to primary care providers.
Impact: These findings may inform organizational-level interventions to improve FOBT(+) follow-up.
©2014 American Association for Cancer Research.
References
-
- American Cancer Society. Cancer Facts and Figures 2013. Atlanta: American Cancer Society; 2013.
-
- Levin B, Lieberman DA, McFarland B, Andrews KS, Brooks D, Bond J, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008 May;134(5):1570–95. - PubMed
-
- Rex DK, Johnson DA, Anderson JC, Schoenfeld PS, Burke CA, Inadomi JM. American College of Gastroenterology guidelines for colorectal cancer screening 2009 [corrected] Am J Gastroenterol. 2009 Mar;104(3):739–50. - PubMed
-
- USPSTF. Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2008 Nov 4;149(9):627–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
