

Chronic Obstructive Pulmonary Disease heterogeneity: challenges for health risk assessment, stratification and management
- PMID: 25472887
- PMCID: PMC4255905
- DOI: 10.1186/1479-5876-12-S2-S3
Chronic Obstructive Pulmonary Disease heterogeneity: challenges for health risk assessment, stratification and management
Abstract
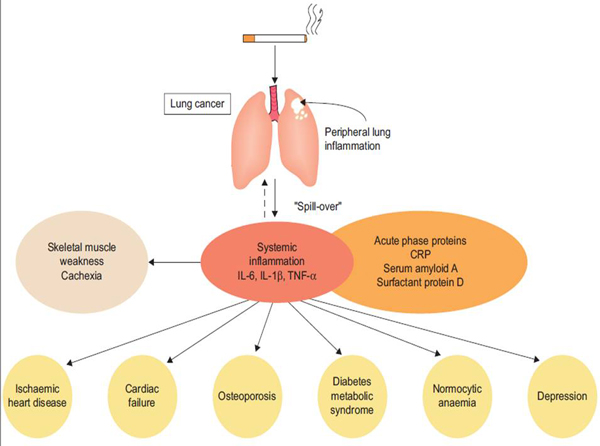
Background and hypothesis: Heterogeneity in clinical manifestations and disease progression in Chronic Obstructive Pulmonary Disease (COPD) lead to consequences for patient health risk assessment, stratification and management. Implicit with the classical "spill over" hypothesis is that COPD heterogeneity is driven by the pulmonary events of the disease. Alternatively, we hypothesized that COPD heterogeneities result from the interplay of mechanisms governing three conceptually different phenomena: 1) pulmonary disease, 2) systemic effects of COPD and 3) co-morbidity clustering, each of them with their own dynamics.
Objective and method: To explore the potential of a systems analysis of COPD heterogeneity focused on skeletal muscle dysfunction and on co-morbidity clustering aiming at generating predictive modeling with impact on patient management. To this end, strategies combining deterministic modeling and network medicine analyses of the Biobridge dataset were used to investigate the mechanisms of skeletal muscle dysfunction. An independent data driven analysis of co-morbidity clustering examining associated genes and pathways was performed using a large dataset (ICD9-CM data from Medicare, 13 million people). Finally, a targeted network analysis using the outcomes of the two approaches (skeletal muscle dysfunction and co-morbidity clustering) explored shared pathways between these phenomena.
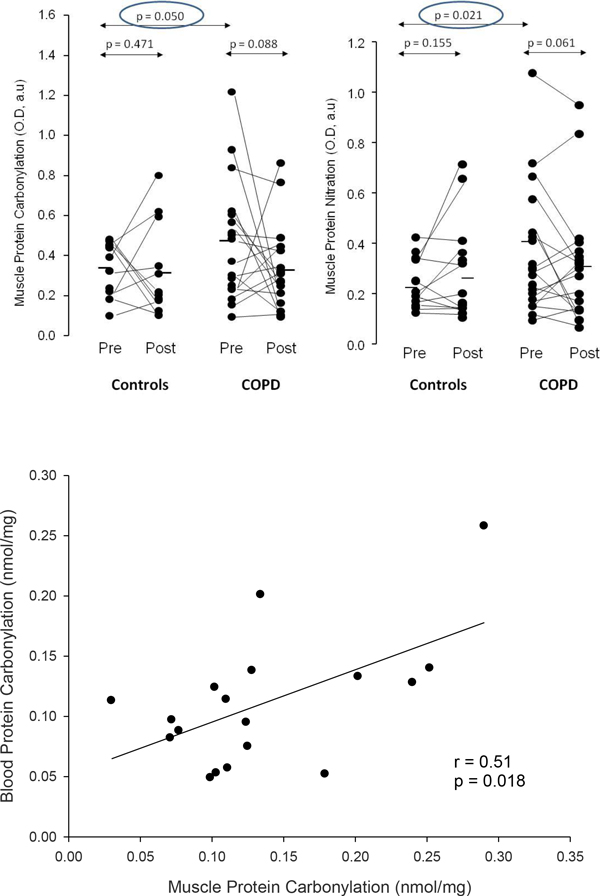
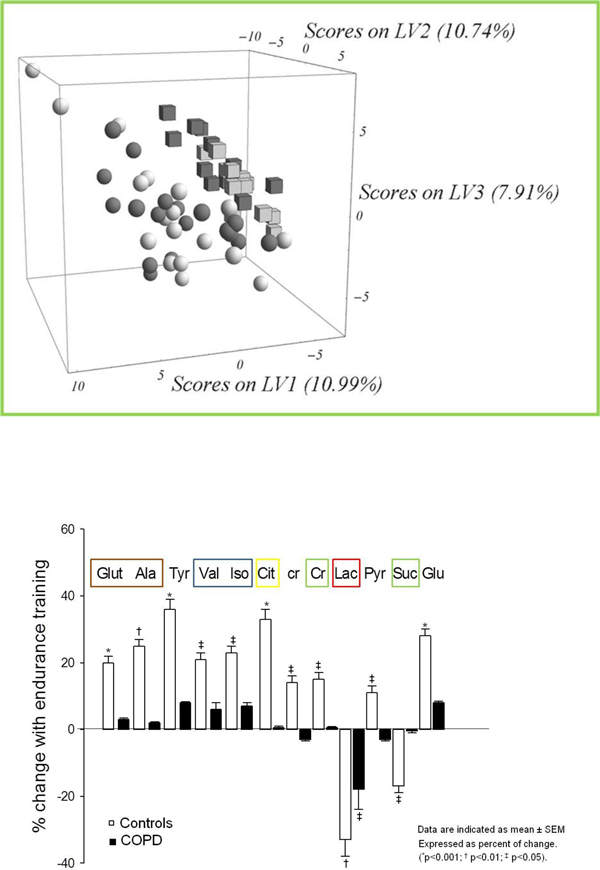
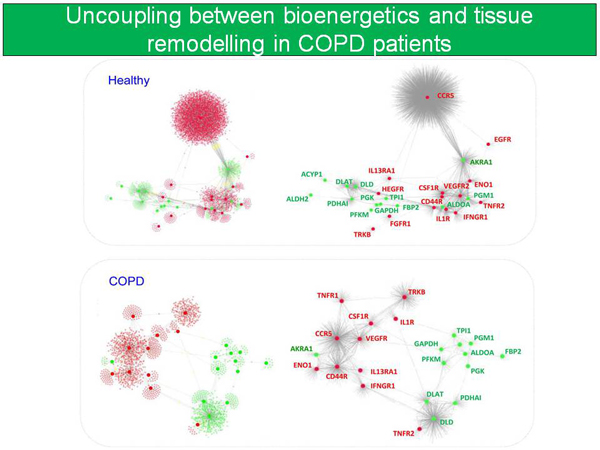
Results: (1) Evidence of abnormal regulation of skeletal muscle bioenergetics and skeletal muscle remodeling showing a significant association with nitroso-redox disequilibrium was observed in COPD; (2) COPD patients presented higher risk for co-morbidity clustering than non-COPD patients increasing with ageing; and, (3) the on-going targeted network analyses suggests shared pathways between skeletal muscle dysfunction and co-morbidity clustering.
Conclusions: The results indicate the high potential of a systems approach to address COPD heterogeneity. Significant knowledge gaps were identified that are relevant to shape strategies aiming at fostering 4P Medicine for patients with COPD.
Figures

References
-
- Vestbo J, Hurd SS, Agusti AG, Jones PW, Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ, Nishimura M, Stockley RA, Sin DD, Rodriguez-Roisin R. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. American journal of respiratory and critical care medicine. 2013;187:347–365. doi: 10.1164/rccm.201204-0596PP. - DOI - PubMed
-
- WHO. 2008-2013 Action Plan for the Global Strategy for the Prevention and Control of Noncommunicable Diseases. 2008. http://www.who.int/nmh/publications/9789241597418/en/ Accessed: 2013-08-20. (Archived by WebCite® at http://www.webcitation.org/6J0XGnHcJ.
-
- Casanova C, de Torres JP, Aguirre-Jaime A, Pinto-Plata V, Marin JM, Cordoba E, Baz R, Cote C, Celli BR. The progression of chronic obstructive pulmonary disease is heterogeneous: the experience of the BODE cohort. American journal of respiratory and critical care medicine. 2011;184:1015–1021. doi: 10.1164/rccm.201105-0831OC. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
