

ACE inhibitors potently reduce vascular inflammation, results of an open proof-of-concept study in the abdominal aortic aneurysm
- PMID: 25474105
- PMCID: PMC4256371
- DOI: 10.1371/journal.pone.0111952
ACE inhibitors potently reduce vascular inflammation, results of an open proof-of-concept study in the abdominal aortic aneurysm
Abstract
Background: Independent of their blood pressure lowering effect, ACE inhibitors are thought to reduce vascular inflammation. The clinical relevance of this effect is unclear with the current knowledge. Abdominal aortic aneurysms (AAA) are characterized by a broad, non-specific inflammatory response, and thus provide a clinical platform to evaluate the anti-inflammatory potential of ACE inhibitors.
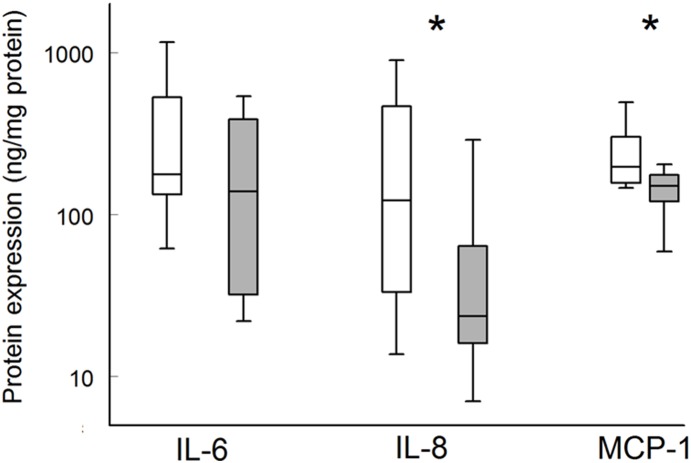
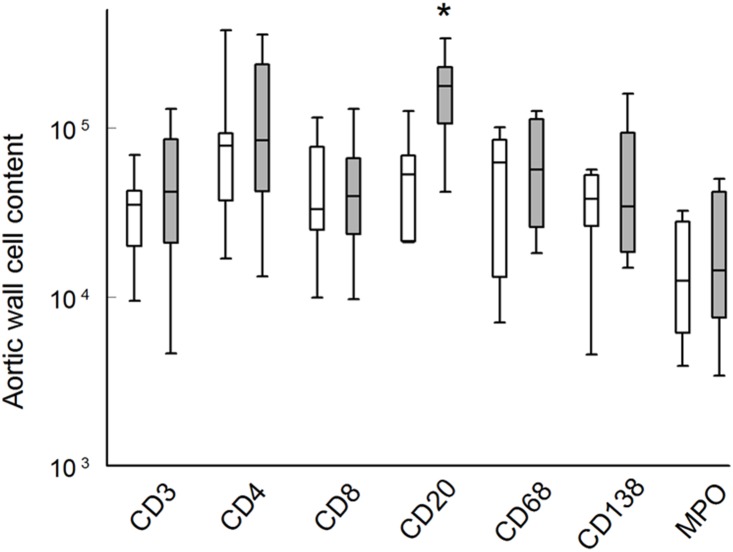
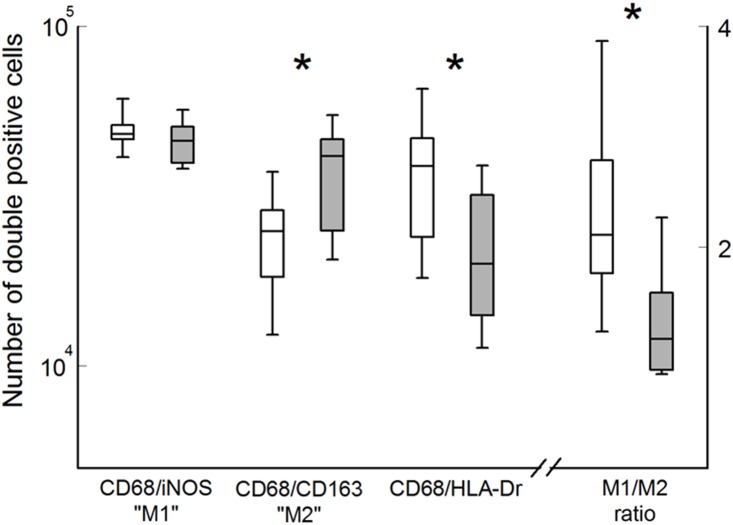
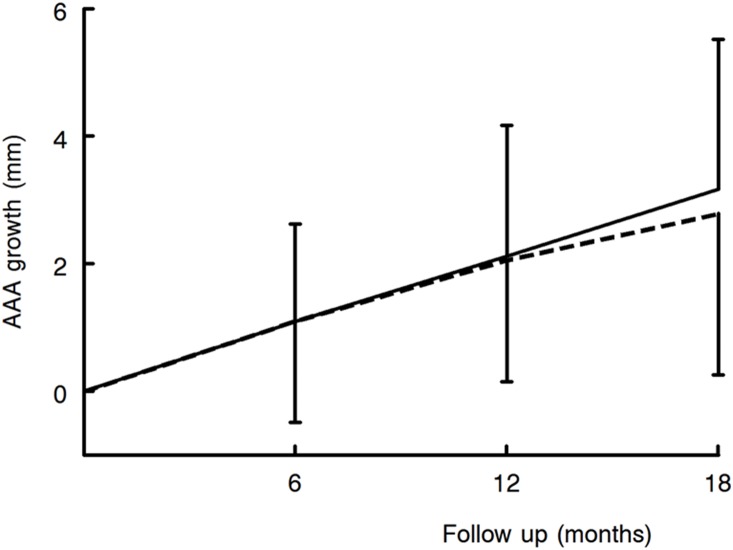
Methods and results: Eleven patients scheduled for open AAA repair received ramipril (5 mg/day) during 2-4 weeks preceding surgery. Aortic wall samples were collected during surgery, and compared to matched samples obtained from a biobank. An anti-inflammatory potential was evaluated in a comprehensive analysis that included immunohistochemistry, mRNA and protein analysis. A putative effect of ACE inhibitors on AAA growth was tested separately by comparing 18-month growth rate of patients on ACE inhibitors (n = 82) and those not taking ACE inhibitors (n = 204). Ramipril reduces mRNA expression of multiple pro-inflammatory cytokines such as IL-1β, IL-6, IL-8, TNF -α, Interferon-[Formula: see text], and MCP-1, as well as aortic wall IL-8 and MCP-1 (P = 0.017 and 0.008, respectively) protein content. The is followed by clear effects on cell activation that included a shift towards anti-inflammatory macrophage (M2) subtype. Evaluation of data from the PHAST cohort did not indicate an effect of ACE inhibitors on 18-month aneurysm progression (mean difference at 18 months: -0.24 mm (95% CI: -0.90-0.45, P = NS).
Conclusions: ACE inhibition quenches multiple aspects of vascular inflammation in AAA. However, this does not translate into reduced aneurysm growth.
Trial registration: Nederlands Trial Register 1345.
Conflict of interest statement
Figures
Similar articles
-
A clinical evaluation of statin pleiotropy: statins selectively and dose-dependently reduce vascular inflammation.PLoS One. 2013;8(1):e53882. doi: 10.1371/journal.pone.0053882. Epub 2013 Jan 22. PLoS One. 2013. PMID: 23349755 Free PMC article. Clinical Trial.
-
The pathophysiology of abdominal aortic aneurysm growth: corresponding and discordant inflammatory and proteolytic processes in abdominal aortic and popliteal artery aneurysms.J Vasc Surg. 2010 Jun;51(6):1479-87. doi: 10.1016/j.jvs.2010.01.057. J Vasc Surg. 2010. PMID: 20488324
-
Hepatocyte growth factor promotes an anti-inflammatory cytokine profile in human abdominal aortic aneurysm tissue.Atherosclerosis. 2011 Jun;216(2):307-12. doi: 10.1016/j.atherosclerosis.2011.02.025. Epub 2011 Feb 24. Atherosclerosis. 2011. PMID: 21411099
-
Novel insight into the pathobiology of abdominal aortic aneurysm and potential future treatment concepts.Prog Cardiovasc Dis. 2007 Nov-Dec;50(3):209-17. doi: 10.1016/j.pcad.2007.05.001. Prog Cardiovasc Dis. 2007. PMID: 17976505 Review.
-
Current status of medical treatment for abdominal aortic aneurysm.Circ J. 2013;77(12):2860-6. doi: 10.1253/circj.cj-13-1252. Epub 2013 Oct 26. Circ J. 2013. PMID: 24161907 Review.
Cited by
-
Sars-Cov2 Induced Biochemical Mechanisms in Liver Damage and Intestinal Lesions.Indian J Clin Biochem. 2022 Nov 12;38(4):1-10. doi: 10.1007/s12291-022-01089-x. Online ahead of print. Indian J Clin Biochem. 2022. PMID: 36407686 Free PMC article.
-
Neuroinflammation in Post-Traumatic Stress Disorder.Biomedicines. 2022 Apr 20;10(5):953. doi: 10.3390/biomedicines10050953. Biomedicines. 2022. PMID: 35625690 Free PMC article. Review.
-
An evaluation of the effect of an angiotensin-converting enzyme inhibitor on the growth rate of small abdominal aortic aneurysms: a randomized placebo-controlled trial (AARDVARK).Eur Heart J. 2016 Nov 7;37(42):3213-3221. doi: 10.1093/eurheartj/ehw257. Epub 2016 Jul 1. Eur Heart J. 2016. PMID: 27371719 Free PMC article. Clinical Trial.
-
Distinctive Under-Expression Profile of Inflammatory and Redox Genes in the Blood of Elderly Patients with Cardiovascular Disease.J Inflamm Res. 2021 Feb 18;14:429-442. doi: 10.2147/JIR.S280328. eCollection 2021. J Inflamm Res. 2021. PMID: 33658823 Free PMC article.
-
Perivascular adipose tissue as a regulator of vascular disease pathogenesis: identifying novel therapeutic targets.Br J Pharmacol. 2017 Oct;174(20):3411-3424. doi: 10.1111/bph.13666. Epub 2016 Dec 14. Br J Pharmacol. 2017. PMID: 27976387 Free PMC article. Review.
References
-
- Krysiak R, Okopien B (2008) Pleiotropic effects of angiotensin-converting enzyme inhibitors in normotensive patients with coronary artery disease. Pharmacol Rep 60:514–523. - PubMed
-
- Xiong F, Zhao J, Zeng G, Huang B, Yuan D, et al. (2014) Inhibition of AAA in a rat model by treatment with ACEI perindopril. J Surg Res 189:166–73. - PubMed
-
- Ruiz-Ortega M, Lorenzo O, Ruperez M, Egido J (2000) ACE inhibitors and AT(1) receptor antagonists-beyond the haemodynamic effect. Nephrol Dial Transplant 15:561–5. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
