

Reproducibility of native myocardial T1 mapping in the assessment of Fabry disease and its role in early detection of cardiac involvement by cardiovascular magnetic resonance
- PMID: 25475749
- PMCID: PMC4256727
- DOI: 10.1186/s12968-014-0099-4
Reproducibility of native myocardial T1 mapping in the assessment of Fabry disease and its role in early detection of cardiac involvement by cardiovascular magnetic resonance
Abstract
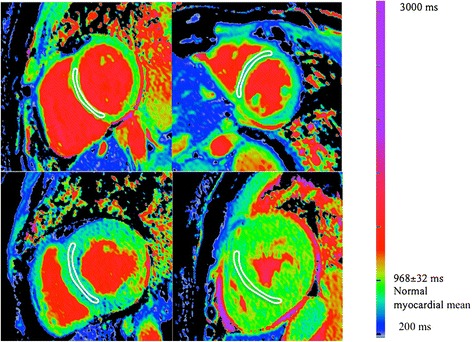
Background: Cardiovascular magnetic resonance (CMR) derived native myocardial T1 is decreased in patients with Fabry disease even before left ventricular hypertrophy (LVH) occurs and may be the first non-invasive measure of myocyte sphingolipid storage. The relationship of native T1 lowering prior to hypertrophy and other candidate early phenotype markers are unknown. Furthermore, the reproducibility of T1 mapping has never been assessed in Fabry disease.
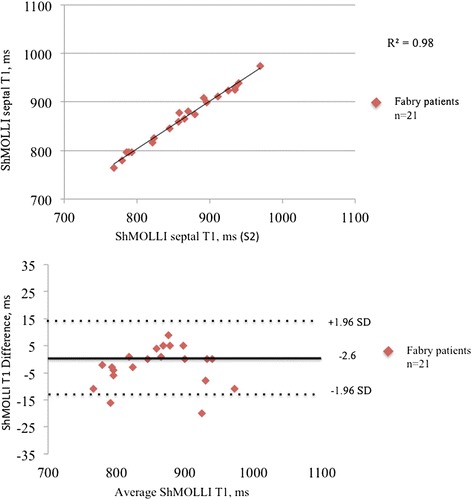
Methods: Sixty-three patients, 34 (54%) female, mean age 48±15 years with confirmed (genotyped) Fabry disease underwent CMR, ECG and echocardiographic assessment. LVH was absent in 25 (40%) patients. Native T1 mapping was performed with both Modified Look-Locker Inversion recovery (MOLLI) sequences and a shortened version (ShMOLLI) at 1.5 Tesla. Twenty-one patients underwent a second scan within 24 hours to assess inter-study reproducibility. Results were compared with 63 healthy age and gender-matched volunteers.
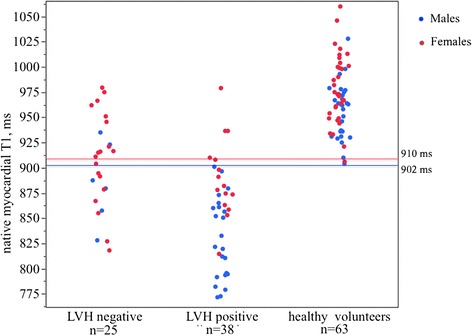
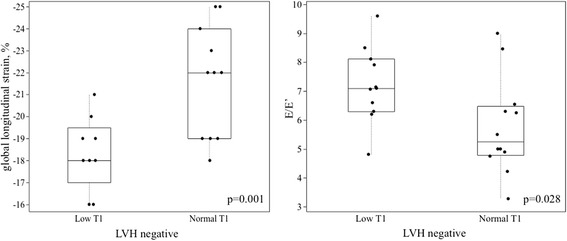
Results: Mean native T1 in Fabry disease (LVH positive), (LVH negative) and healthy volunteers was 853±50 ms, 904±46 ms and 968±32 ms (for all p<0.0001) by ShMOLLI sequences. Native T1 showed high inter-study, intra-observer and inter-observer agreement with intra-class correlation coefficients (ICC) of 0.99, 0.98, 0.97 (ShMOLLI) and 0.98, 0.98, 0.98 (MOLLI). In Fabry disease LVH negative individuals, low native T1 was associated with reduced echocardiographic-based global longitudinal speckle tracking strain (-18±2% vs -22±2%, p=0.001) and early diastolic function impairment (E/E'=7 [6-8] vs 5 [5-6], p=0.028).
Conclusion: Native T1 mapping in Fabry disease is a reproducible technique. T1 reduction prior to the onset of LVH is associated with early diastolic and systolic changes measured by echocardiography.
Figures
Similar articles
-
Loss of base-to-apex circumferential strain gradient assessed by cardiovascular magnetic resonance in Fabry disease: relationship to T1 mapping, late gadolinium enhancement and hypertrophy.J Cardiovasc Magn Reson. 2019 Aug 1;21(1):45. doi: 10.1186/s12968-019-0557-0. J Cardiovasc Magn Reson. 2019. PMID: 31366357 Free PMC article.
-
Systolic and diastolic function assessment in fabry disease patients using speckle-tracking imaging and comparison with conventional echocardiographic measurements.J Am Soc Echocardiogr. 2013 Dec;26(12):1407-14. doi: 10.1016/j.echo.2013.09.005. Epub 2013 Oct 11. J Am Soc Echocardiogr. 2013. PMID: 24125876
-
Identification and assessment of Anderson-Fabry disease by cardiovascular magnetic resonance noncontrast myocardial T1 mapping.Circ Cardiovasc Imaging. 2013 May 1;6(3):392-8. doi: 10.1161/CIRCIMAGING.112.000070. Epub 2013 Apr 5. Circ Cardiovasc Imaging. 2013. PMID: 23564562
-
Proposed Stages of Myocardial Phenotype Development in Fabry Disease.JACC Cardiovasc Imaging. 2019 Aug;12(8 Pt 2):1673-1683. doi: 10.1016/j.jcmg.2018.03.020. Epub 2018 May 16. JACC Cardiovasc Imaging. 2019. PMID: 29778854
-
[Cardiological follow-up in patients with Fabry disease].G Ital Cardiol (Rome). 2010 Jul-Aug;11(7-8):566-72. G Ital Cardiol (Rome). 2010. PMID: 21033333 Review. Italian.
Cited by
-
Myocardial T1 and T2 Mapping: Techniques and Clinical Applications.Korean J Radiol. 2017 Jan-Feb;18(1):113-131. doi: 10.3348/kjr.2017.18.1.113. Epub 2017 Jan 5. Korean J Radiol. 2017. PMID: 28096723 Free PMC article. Review.
-
Impact of cardiac magnetic resonance imaging in non-ischemic cardiomyopathies.World J Cardiol. 2016 Feb 26;8(2):132-45. doi: 10.4330/wjc.v8.i2.132. World J Cardiol. 2016. PMID: 26981210 Free PMC article. Review.
-
Cardiac Manifestations in Fabry Disease: A Case Report on Two Siblings.Diagnostics (Basel). 2025 Jan 31;15(3):340. doi: 10.3390/diagnostics15030340. Diagnostics (Basel). 2025. PMID: 39941270 Free PMC article.
-
Magnetic resonance imaging phantoms for quality-control of myocardial T1 and ECV mapping: specific formulation, long-term stability and variation with heart rate and temperature.J Cardiovasc Magn Reson. 2016 Sep 22;18(1):62. doi: 10.1186/s12968-016-0275-9. J Cardiovasc Magn Reson. 2016. PMID: 27659737 Free PMC article.
-
Imaging predictors of adverse prognosis in Fabry disease cardiomyopathy: A systematic review and meta-analysis.Eur J Clin Invest. 2025 May;55(5):e14388. doi: 10.1111/eci.14388. Epub 2025 Jan 22. Eur J Clin Invest. 2025. PMID: 39840688 Free PMC article.
References
-
- Hughes DA, Elliott PM, Shah J, Zuckerman J, Coghlan G, Brookes J, Mehta AB. Effects of enzyme replacement therapy on the cardiomyopathy of anderson-fabry disease: a randomised, double-blind, placebo-controlled clinical trial of agalsidase alfa. Heart. 2008;94(2):153–158. doi: 10.1136/hrt.2006.104026. - DOI - PubMed
-
- Moon JC, Sachdev B, Elkington AG, McKenna WJ, Mehta A, Pennell DJ, Leed PJ, Elliott PM. Gadolinium enhanced cardiovascular magnetic resonance in anderson-fabry disease. Evidence for a disease specific abnormality of the myocardial interstitium. Eur Heart J. 2003;24:2151–2155. doi: 10.1016/j.ehj.2003.09.017. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
