

Protecting the confidentiality of interim data: addressing current challenges
- PMID: 25475877
- PMCID: PMC4344915
- DOI: 10.1177/1740774514561243
Protecting the confidentiality of interim data: addressing current challenges
Abstract
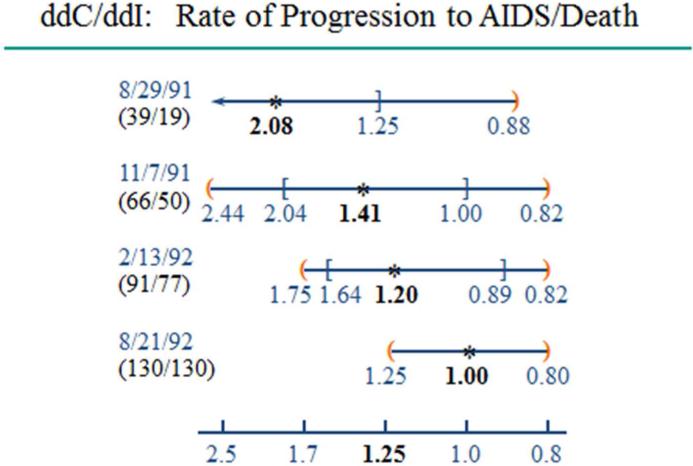
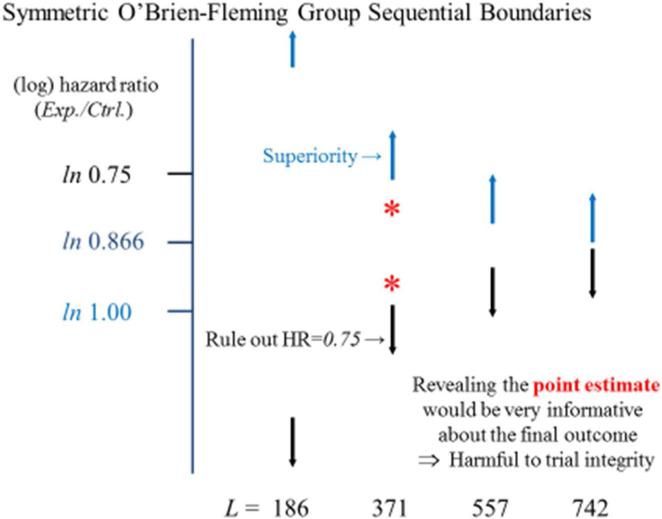
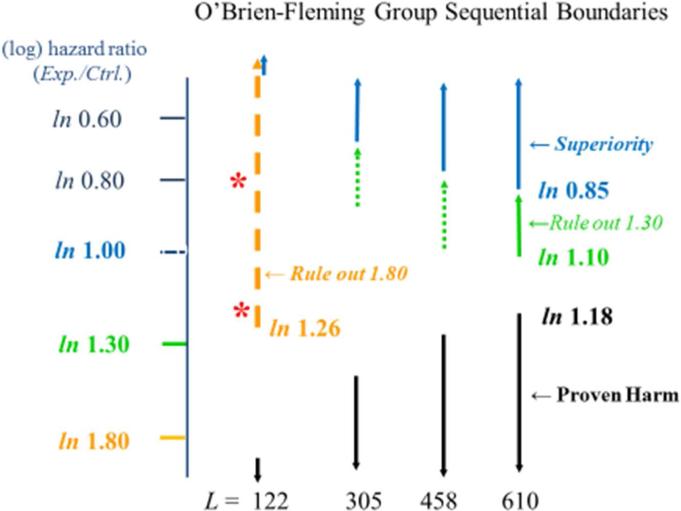
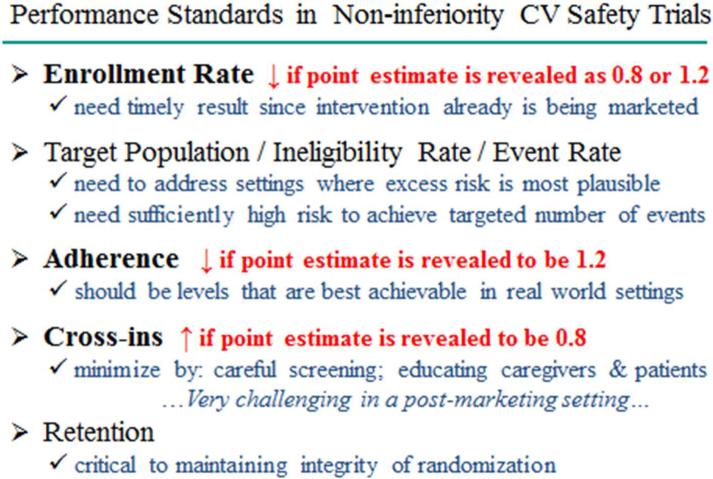
There is compelling evidence supporting the importance of maintaining confidentiality of interim data in clinical trials designed to reliably address the benefit-to-risk profile of interventions. While this is widely recognized, creative approaches are needed to achieve this in challenging settings where interim data are released for regulatory review and action, even though the trial would be continued to address its primary hypothesis. An illustration is the recently emerging setting of cardiovascular safety trials in type 2 diabetes mellitus. At the first stage of such trials, if large relative increases in cardiovascular major morbidity/mortality can be ruled out, data can be released solely for the purpose of allowing regulatory decision making about marketing approval. The trial is then continued in the post-marketing setting to address the primary hypothesis regarding whether smaller relative increases can be ruled out. Active rather than passive approaches are needed to protect the integrity of cardiovascular safety trials. Given the importance to trial integrity of maintaining confidentiality of interim data such as the estimated relative effect on cardiovascular risk, a Data Access Plan should be in place in these trials to ensure such data are not revealed to study participants and their caregivers, investigators involved in trial conduct, the sponsor's management team, and the public, until trial completion. A Performance Standards Document also should be developed to pre-specify targeted and minimally acceptable levels for recruitment rate, best real-world achievable adherence, avoidance of cross-ins, and retention rate. This document should specify creative approaches for achieving these targets, oversight procedures during trial conduct to monitor performance levels, and actions to be taken if emerging data indicate minimally acceptable levels are not being reached. In settings where meaningful breaches in confidentiality have occurred, such oversight allows adverse effects on trial integrity to be detected earlier and more effectively addressed.
Keywords: Data Access Plan; Data Monitoring Committee; Performance Standards Document; cardiovascular safety trials.
© The Author(s) 2014.
Figures
Comment in
-
Commentary: preserving confidentiality of interim data.Clin Trials. 2015 Feb;12(1):18-20. doi: 10.1177/1740774514562032. Epub 2014 Dec 5. Clin Trials. 2015. PMID: 25480540 No abstract available.
-
Commentary: confidentiality of interim trial data-the emerging crisis.Clin Trials. 2015 Feb;12(1):15-7. doi: 10.1177/1740774514561661. Epub 2014 Dec 18. Clin Trials. 2015. PMID: 25525072 No abstract available.
-
Commentary: data monitoring confidentiality and FDA transparency.Clin Trials. 2015 Feb;12(1):12-4. doi: 10.1177/1740774514561047. Epub 2014 Dec 18. Clin Trials. 2015. PMID: 25525073 No abstract available.
-
Response.Clin Trials. 2015 Feb;12(1):21-3. doi: 10.1177/1740774514563356. Clin Trials. 2015. PMID: 25721147 No abstract available.
References
-
- Ellenberg S, Fleming T, DeMets D. Data monitoring committees in clinical trials: A practical perspective. John Wiley & Sons, Ltd; West Sussex, England: 2002.
-
- Grant AM, Altman DG, Babiker AB, et al. Issues in data monitoring and interim analyses of trials. Health Technol Assess. 2005;9:25. - PubMed
-
- Green SJ, Fleming TR, O'Fallon JR. Policies for study monitoring and interim reporting of results. Journal Clin Oncol. 1987;5:2477–2484. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
