

Improved human observer performance in digital reconstructed radiograph verification in head and neck cancer radiotherapy
- PMID: 25477277
- PMCID: PMC4801514
- DOI: 10.1007/s11548-014-1127-4
Improved human observer performance in digital reconstructed radiograph verification in head and neck cancer radiotherapy
Abstract
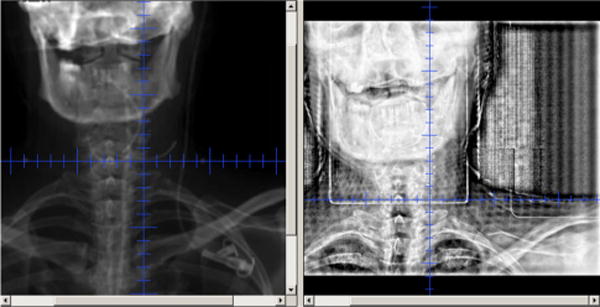
Purpose: Digitally reconstructed radiographs (DRRs) are routinely used as an a priori reference for setup correction in radiotherapy. The spatial resolution of DRRs may be improved to reduce setup error in fractionated radiotherapy treatment protocols. The influence of finer CT slice thickness reconstruction (STR) and resultant increased resolution DRRs on physician setup accuracy was prospectively evaluated.
Methods: Four head and neck patient CT-simulation images were acquired and used to create DRR cohorts by varying STRs at 0.5, 1, 2, 2.5, and 3 mm. DRRs were displaced relative to a fixed isocenter using 0-5 mm random shifts in the three cardinal axes. Physician observers reviewed DRRs of varying STRs and displacements and then aligned reference and test DRRs replicating daily KV imaging workflow. A total of 1,064 images were reviewed by four blinded physicians. Observer errors were analyzed using nonparametric statistics (Friedman's test) to determine whether STR cohorts had detectably different displacement profiles. Post hoc bootstrap resampling was applied to evaluate potential generalizability.
Results: The observer-based trial revealed a statistically significant difference between cohort means for observer displacement vector error ([Formula: see text]) and for [Formula: see text]-axis [Formula: see text]. Bootstrap analysis suggests a 15% gain in isocenter translational setup error with reduction of STR from 3 mm to [Formula: see text]2 mm, though interobserver variance was a larger feature than STR-associated measurement variance.
Conclusions: Higher resolution DRRs generated using finer CT scan STR resulted in improved observer performance at shift detection and could decrease operator-dependent geometric error. Ideally, CT STRs [Formula: see text]2 mm should be utilized for DRR generation in the head and neck.
Keywords: IGRT; Image informatics; Image-guided radiotherapy; Quality assurance; Setup error.
Conflict of interest statement
Figures



References
-
- Chen AM, Farwell DG, Luu Q, Donald PJ, Perks J, Purdy JA. Evaluation of the planning target volume in the treatment of head and neck cancer with intensity-modulated radiotherapy: what is the appropriate expansion margin in the setting of daily image guidance? Int J Radiat Oncol Biol Phys. 2011;81(4):943–949. doi: 10.1016/j.ijrobp.2010.07.017. - DOI - PubMed
-
- Serago CF, Buskirk SJ, Igel TC, Gale AA, Serago NE, Earle JD. Comparison of daily megavoltage electronic portal imaging or kilovoltage imaging with marker seeds to ultrasound imaging or skin marks for prostate localization and treatment positioning in patients with prostate cancer. Int J Radiat Oncol Biol Phys. 2006;65(5):1585–1592. doi: 10.1016/j.ijrobp.2006.04.019. - DOI - PubMed
-
- Fuller CD, Scarbrough TJ, Sonke JJ, Rasch CR, Choi M, Ting JY, Wang SJ, Papanikolaou N, Rosenthal DI. Method comparison of automated matching software-assisted cone-beam CT and stereoscopic kilovoltage x-ray positional verification image-guided radiation therapy for head and neck cancer: a prospective analysis. Phys Med Biol. 2009;54(24):7401–7415. doi: 10.1088/0031-9155/54/24/010. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
