

Diagnosis and early detection of COPD using spirometry
- PMID: 25478197
- PMCID: PMC4255165
- DOI: 10.3978/j.issn.2072-1439.2014.08.18
Diagnosis and early detection of COPD using spirometry
Abstract
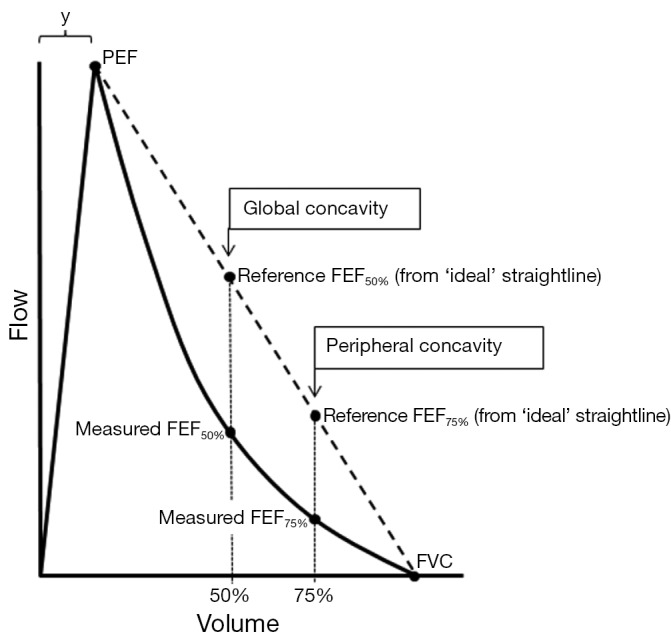
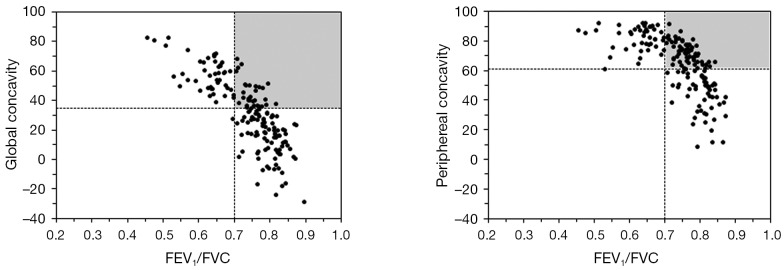
The standard respiratory function test for case detection of chronic obstructive pulmonary disease (COPD) is spirometry. The criterion for diagnosis defined in guidelines is based on the FEV1/FVC ratio forced expiratory ratio (FER) and its severity is based on forced expiratory volume in one second (FEV1) from measurements obtained during maximal forced expiratory manoeuvres. Spirometry is a safe and practical procedure, and when conducted by a trained operator using a spirometer that provides quality feedback, the majority of patients can be coached to provide acceptable and repeatable results. This allows potentially wide application of testing to improve recognition and diagnosis of COPD, such as for case finding in primary care. However, COPD remains substantially under diagnosed in primary care and a major reason for this is underuse of spirometry. The presence of symptoms is not a reliable indicator of disease and diagnosis is often delayed until more severe airflow obstruction is present. Early diagnosis is worthwhile, as it allows risk factors for COPD such as smoking to be addressed promptly and treatment optimised. Paradoxically, investigation of the patho-physiology in COPD has shown that extensive small airway disease exists before it is detectable with conventional spirometric indices, and methods to detect airway disease earlier using the flow-volume curve are discussed.
Keywords: Spirometry; case finding; chronic obstructive pulmonary disease (COPD); flow-volume curve.
Figures
References
-
- Anderson DO, Ferris BG. Role of Tobacco Smoking in the Causation of Chronic Respiratory Disease. N Engl J Med 1962;267:787-94. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical