

Protein-repellent and antibacterial dental composite to inhibit biofilms and caries
- PMID: 25478889
- PMCID: PMC4321720
- DOI: 10.1016/j.jdent.2014.11.008
Protein-repellent and antibacterial dental composite to inhibit biofilms and caries
Abstract
Objectives: Biofilm acids contribute to secondary caries, which is a main reason for dental restoration failures. The objectives of this study were to: (1) develop a protein-repellent and antibacterial composite, and (2) investigate the effects of combining 2-methacryloyloxyethyl phosphorylcholine (MPC) with quaternary ammonium dimethylaminohexadecyl methacrylate (DMAHDM) on composite mechanical properties and biofilm response for the first time.
Methods: MPC, DMAHDM and glass particles were mixed into a dental resin composite. Mechanical properties were measured in three-point flexure. Protein adsorption onto the composites was measured by a micro bicinchoninic acid method. A human saliva microcosm model was used to grow biofilms on composites. Colony-forming unit (CFU) counts, live/dead assay, metabolic activity, and lactic acid production of biofilms were determined.
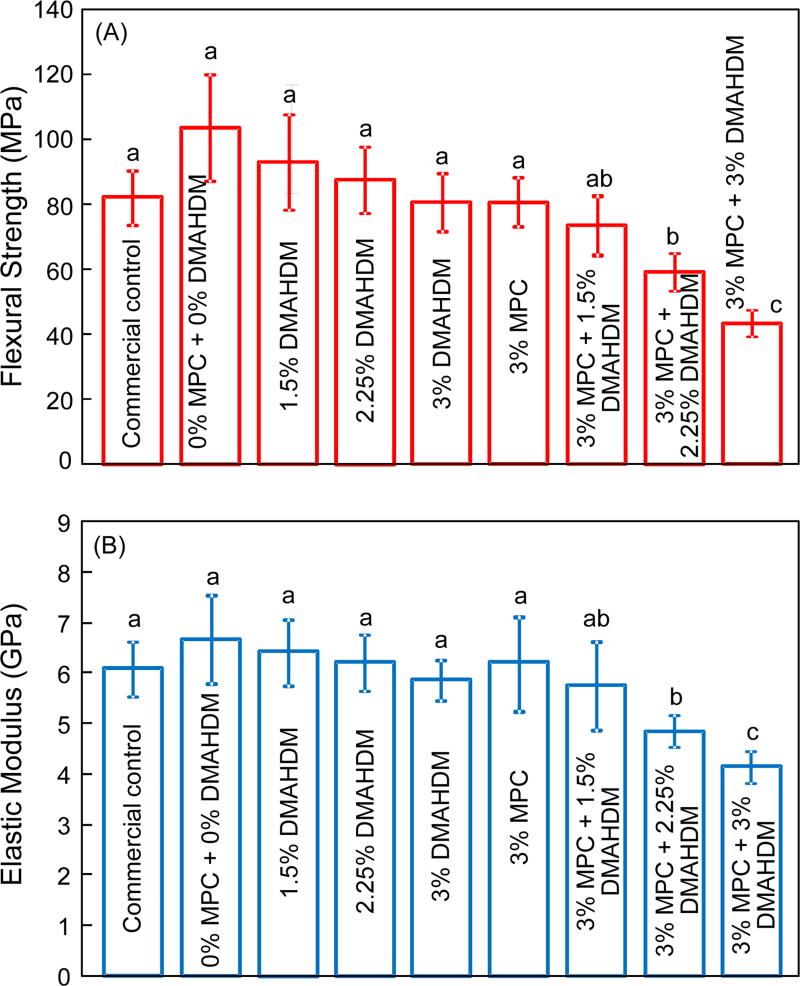
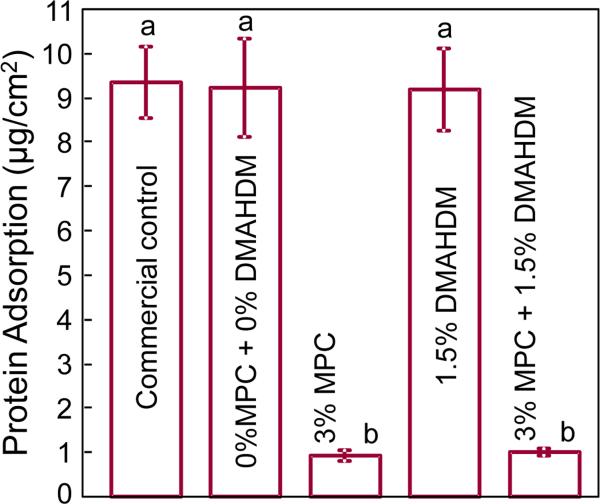
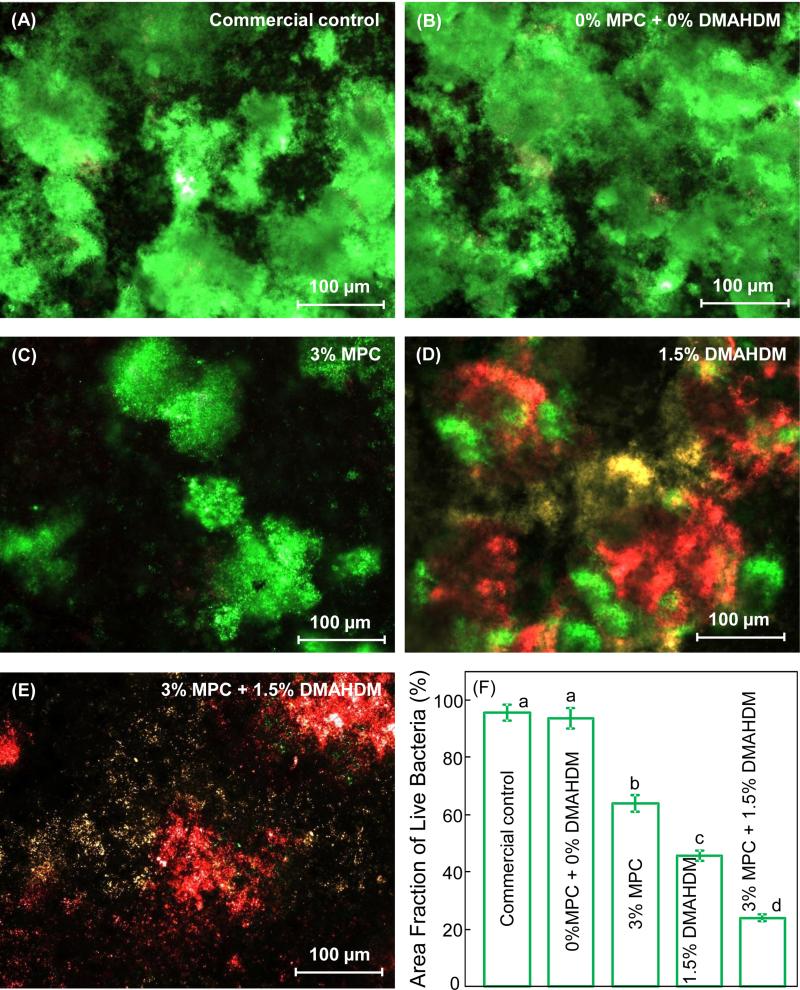
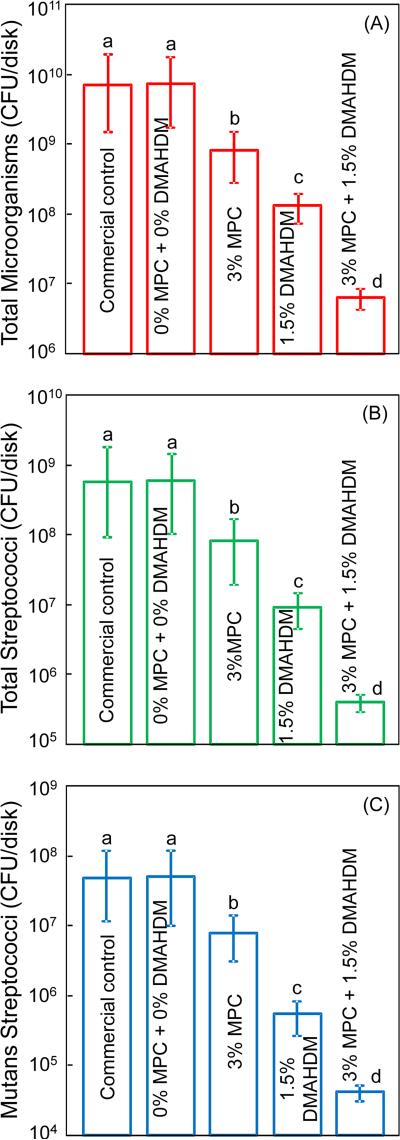
Results: Incorporation of 3% MPC and 1.5% DMAHDM into composite achieved protein-repellent and antibacterial capabilities without compromising the mechanical properties. Composite with 3% MPC+1.5% DMAHDM had protein adsorption that was 1/10 that of a commercial composite (p<0.05). The composite with 3% MPC+1.5% DMAHDM had much greater reduction in biofilm growth than using MPC or DMAHDM alone (p<0.05). Biofilm CFU counts on composite with 3% MPC+1.5% DMAHDM were more than three orders of magnitude lower than that of commercial control.
Conclusions: Dental composite with a combination of strong protein-repellent and antibacterial capabilities was developed for the first time. Composite containing MPC and DMAHDM greatly reduced biofilm growth and lactic acid production, without compromising mechanical properties of the composite.
Clinical significance: Novel composite with MPC and DMAHDM greatly reduced biofilm activity and is promising to inhibit secondary caries. The dual agents of MPC plus DMAHDM may have wide applicability to other dental materials.
Keywords: Antibacterial property; Caries inhibition; Human saliva microcosm biofilm; Mechanical property; Protein repellent; Resin composite.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures

Similar articles
-
Effects of Long-Term Water-Aging on Novel Anti-Biofilm and Protein-Repellent Dental Composite.Int J Mol Sci. 2017 Jan 18;18(1):186. doi: 10.3390/ijms18010186. Int J Mol Sci. 2017. PMID: 28106774 Free PMC article.
-
Development of novel dental adhesive with double benefits of protein-repellent and antibacterial capabilities.Dent Mater. 2015 Jul;31(7):845-54. doi: 10.1016/j.dental.2015.04.013. Epub 2015 May 17. Dent Mater. 2015. PMID: 25990262
-
Protein-repellent and antibacterial functions of a calcium phosphate rechargeable nanocomposite.J Dent. 2016 Sep;52:15-22. doi: 10.1016/j.jdent.2016.06.003. Epub 2016 Jun 17. J Dent. 2016. PMID: 27327110
-
Nanostructured Polymeric Materials with Protein-Repellent and Anti-Caries Properties for Dental Applications.Nanomaterials (Basel). 2018 Jun 1;8(6):393. doi: 10.3390/nano8060393. Nanomaterials (Basel). 2018. PMID: 29865184 Free PMC article. Review.
-
Dental restorative materials containing quaternary ammonium compounds have sustained antibacterial action.J Am Dent Assoc. 2022 Dec;153(12):1114-1120. doi: 10.1016/j.adaj.2022.09.006. Epub 2022 Oct 20. J Am Dent Assoc. 2022. PMID: 36272816 Review.
Cited by
-
Recent Advances in Quaternary Ammonium Monomers for Dental Applications.Materials (Basel). 2024 Jan 10;17(2):345. doi: 10.3390/ma17020345. Materials (Basel). 2024. PMID: 38255513 Free PMC article. Review.
-
The Influence of 2-Methacryloyloxyethyl Phosphorylcholine Polymer Materials on Orthodontic Friction and Attachment of Oral Bacteria.Materials (Basel). 2022 Aug 21;15(16):5770. doi: 10.3390/ma15165770. Materials (Basel). 2022. PMID: 36013906 Free PMC article.
-
Recent Advances in the Development of Antimicrobial and Antifouling Biocompatible Materials for Dental Applications.Materials (Basel). 2021 Jun 9;14(12):3167. doi: 10.3390/ma14123167. Materials (Basel). 2021. PMID: 34207552 Free PMC article. Review.
-
Antibacterial and protein-repellent orthodontic cement to combat biofilms and white spot lesions.J Dent. 2015 Dec;43(12):1529-38. doi: 10.1016/j.jdent.2015.09.006. Epub 2015 Sep 30. J Dent. 2015. PMID: 26427311 Free PMC article.
-
Bio-Interactive Zwitterionic Dental Biomaterials for Improving Biofilm Resistance: Characteristics and Applications.Int J Mol Sci. 2020 Nov 29;21(23):9087. doi: 10.3390/ijms21239087. Int J Mol Sci. 2020. PMID: 33260367 Free PMC article. Review.
References
-
- Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007;369:51–9. - PubMed
-
- Ferracane JL. Resin composite – State of the art. Dental Materials. 2011;27:29–38. - PubMed
-
- Lim BS, Ferracane JL, Sakaguchi RL, Condon JR. Reduction of polymerization contraction stress for dental composites by two-step light-activation. Dental Materials. 2002;18:436–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
