

Potential for large outbreaks of Ebola virus disease
- PMID: 25480136
- PMCID: PMC4255970
- DOI: 10.1016/j.epidem.2014.09.003
Potential for large outbreaks of Ebola virus disease
Abstract
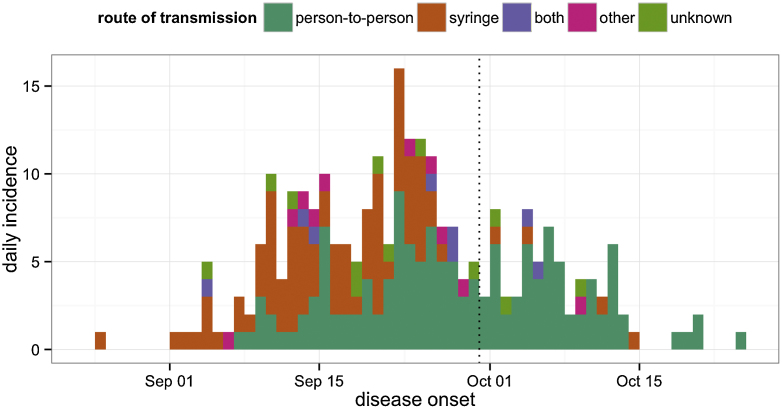
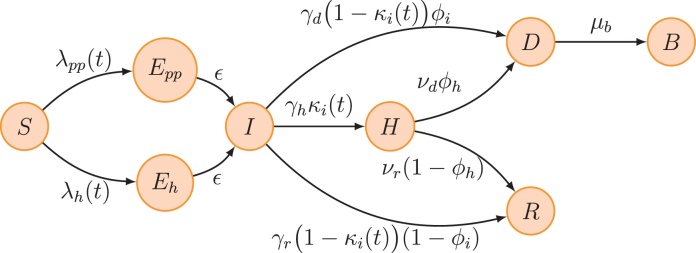
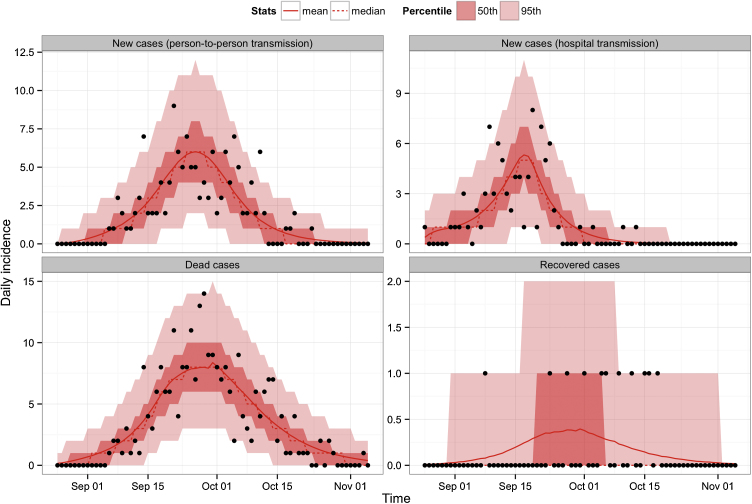
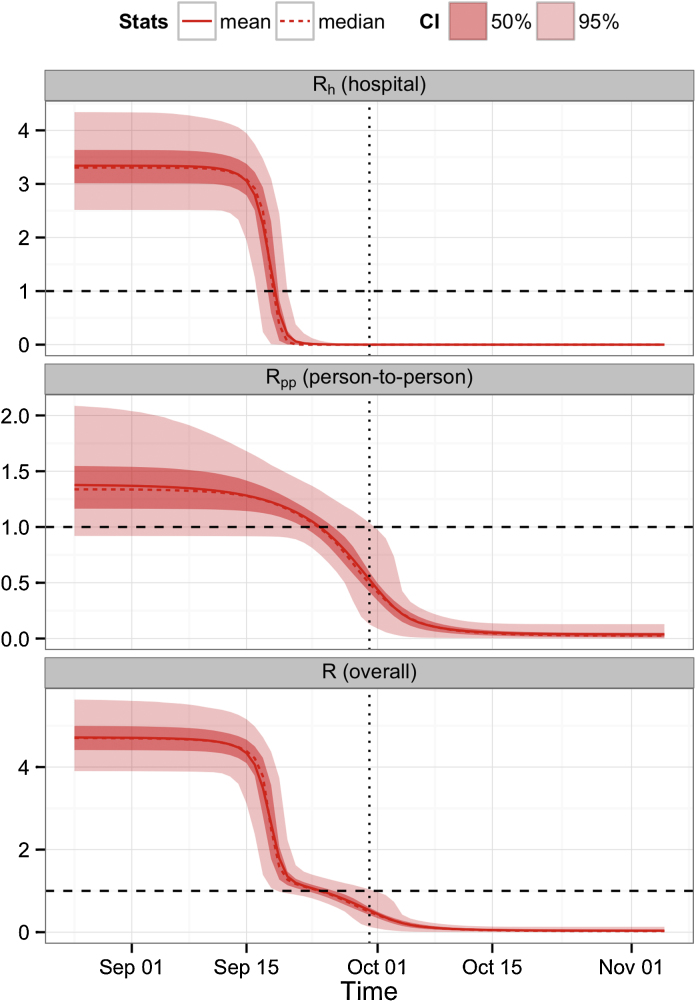
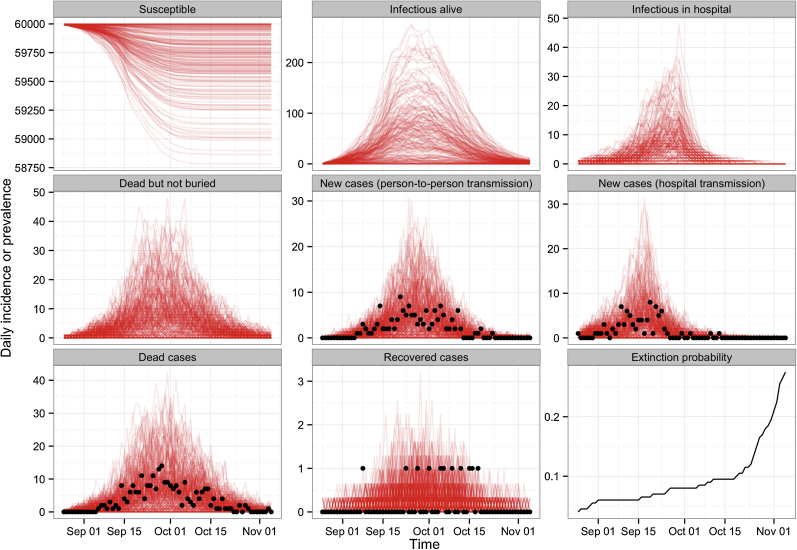
Outbreaks of Ebola virus can cause substantial morbidity and mortality in affected regions. The largest outbreak of Ebola to date is currently underway in West Africa, with 3944 cases reported as of 5th September 2014. To develop a better understanding of Ebola transmission dynamics, we revisited data from the first known Ebola outbreak, which occurred in 1976 in Zaire (now Democratic Republic of Congo). By fitting a mathematical model to time series stratified by disease onset, outcome and source of infection, we were able to estimate several epidemiological quantities that have previously proved challenging to measure, including the contribution of hospital and community infection to transmission. We found evidence that transmission decreased considerably before the closure of the hospital, suggesting that the decline of the outbreak was most likely the result of changes in host behaviour. Our analysis suggests that the person-to-person reproduction number was 1.34 (95% CI: 0.92-2.11) in the early part of the outbreak. Using stochastic simulations we demonstrate that the same epidemiological conditions that were present in 1976 could have generated a large outbreak purely by chance. At the same time, the relatively high person-to-person basic reproduction number suggests that Ebola would have been difficult to control through hospital-based infection control measures alone.
Keywords: 1976 Zaire outbreak; Basic reproduction number; Ebola; Mathematical model.
Copyright © 2014 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Baize S., Pannetier D., Oestereich L., Rieger T., Koivogui L., Magassouba N., Soropogui B., Sow M.S., Keï ta S., De Clerck H., Tiffany A., Dominguez G., Loua M., Traoré A., Kolié M., Malano E.R., Heleze E., Bocquin A., Mély S., Raoul H., Caro V., Cadar D., Gabriel M., Pahlmann M., Tappe D., Schmidt-Chanasit J., Impouma B., Diallo A.K., Formenty P., Van Herp M., Günther S. Emergence of Zaire Ebola Virus Disease in Guinea: Preliminary Report. N. Engl. J. Med. 2014 - PubMed
-
- Breman J., Piot P., Johnson K., White M., Mbuyi M., Sureau P., Heymann D., Van Nieuwenhove S., McCormick J., Ruppol J. The epidemiology of Ebola hemorrhagic fever in Zaire 1976. In: Pattyn S.R., editor. Ebola Virus Haemorrhagic Fever. Elsevier; Amsterdam, The Netherlands: 1978. pp. 85–97.
-
- Centers for Disease Control and Prevention . 2014. Outbreaks Chronology: Ebola Hemorrhagic Fever.http://www.cdc.gov/vhf/ebola/resources/outbreak-table.html
-
- Chowell G., Hengartner N.W., Castillo-Chavez C., Fenimore P.W., Hyman J.M. The basic reproductive number of Ebola and the effects of public health measures: the cases of Congo and Uganda. J. Theor. Biol. 2004;229:119–126. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
