

Occipital calcified pseudoneoplasms of the neuraxis (CAPNON): understanding a rare pathology
- PMID: 25480139
- PMCID: PMC4265027
- DOI: 10.1136/bcr-2014-206855
Occipital calcified pseudoneoplasms of the neuraxis (CAPNON): understanding a rare pathology
Abstract
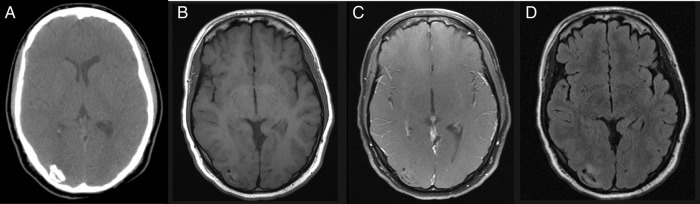
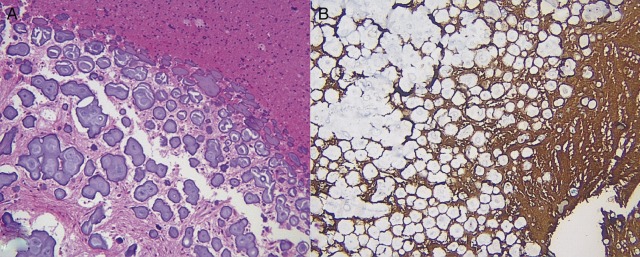
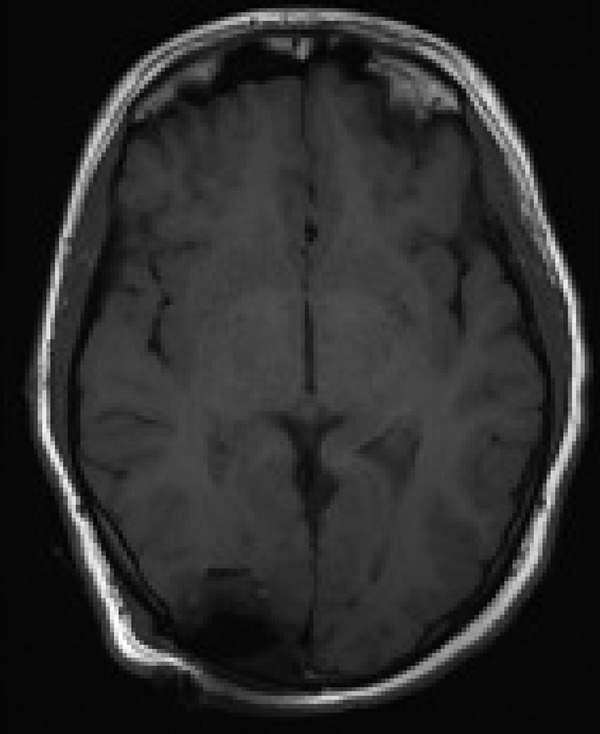
Calcifying pseudoneoplasms of the neuraxis (CAPNON) are rare and typically benign lesions that can occur anywhere within the central nervous system. Aetiology of this lesion is unclear and surgical removal is usually curative. We present a 24-year-old male patient with a history of occipital migraines who was admitted after sudden onset seizure and loss of vision. CT and MRI demonstrated a small calcifying lesion in the right temporo-occipital lobe. The patient underwent gross total resection of the tumour mass and pathological analysis revealed a CAPNON. The preoperative diagnosis of CAPNON remains difficult due to unspecific radiological findings, yet a clear understanding of characteristic pathological findings and prognosis of CAPNON remains paramount.
2014 BMJ Publishing Group Ltd.
Figures
References
-
- Rhodes RH, Davis RL. An unusual fibro-osseous component in intracranial lesions. Hum Pathol 1978;9:309–19. - PubMed
-
- Kerr EE, Borys E, Bobinski M. ,et al. Posterior fossa calcifying pseudoneoplasm of the central nervous system. J Neurosurg 2013;118:896–902. - PubMed
-
- Grabowski M, Recinos P, Chen T et al. . Calcifying pseudoneoplasm of the neuraxis overlying the corpus callosum: a case report and review of the literature. Clin Neuropathol 2013;32:515–21. - PubMed
-
- Stienen MN, Abdulazim A, Gautschi OP et al. . Calcifying pseudoneoplasms of the neuraxis (CAPNON): clinical features and therapeutic options. Acta Neurochir (Wien) 2013;155:9–17. - PubMed
-
- Smith DM, Berry AD III. Unusual fibro-osseous lesion of the spinal cord with positive staining for glial fibrillary acidic protein and radiological progression: a case report. Hum pathol 1994;25:835–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical