

Guided (VENTRI-GUIDE) versus freehand ventriculostomy: study protocol for a randomized controlled trial
- PMID: 25480528
- PMCID: PMC4289205
- DOI: 10.1186/1745-6215-15-478
Guided (VENTRI-GUIDE) versus freehand ventriculostomy: study protocol for a randomized controlled trial
Abstract
Background: Despite the widespread use of external ventricular drainage, revision rates, and associated complications are reported between 10 and 40%. Current available image-guided techniques using stereotaxy, endoscopy, or ultrasound for catheter placements remain time-consuming techniques. Recently, a smartphone-assisted guide with high precision has been described. The development of an easy-to-use, portable, image-guided system could reduce the need for multiple passes and improve the rate of accurate catheter placement. This study aims to prospectively compare in a randomized controlled manner the accuracy of the freehand pass technique versus an easy-to-use, portable, adjustable guiding device for ventriculostomy catheter placement.
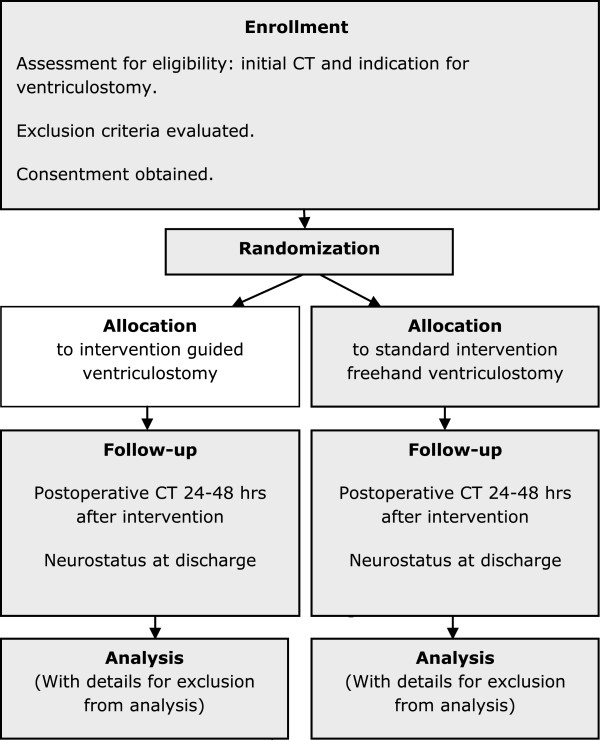
Methods/design: This is a single center, prospective, randomized trial with a blinded endpoint (ventricular catheter tip location) assessment. Adult patients with the indication for ventriculostomy, as proven by computed tomography (CT), will be randomly assigned to the treatment group or the control group. For patients in the treatment group, ventriculostomy will be performed using an adjustable guiding device and DICOM (Digital Imaging and Communications in Medicine) image-reading software assistance (for example, using a mini-tablet) based on preoperative CT imaging.Patients in the control group will receive standard freehand ventriculostomy using anatomical landmarks. The catheter may be placed for external drainage or internal (ventriculoperitoneal) shunting in both groups. The primary outcome measure is the rate of correct placements of the ventricular catheter, defined as a score of 1 to 3 on grading system for catheter tip location on a postoperative CT scan. Participants will be followed for the duration of hospital stay, an expected average of two weeks. The primary outcome will be determined by one of the authors blinded to the treatment allocation. We aim to include 236 patients in three years. Secondary outcome measures include: frequency of placements required, frequency of completed placements within the ventricle of the perforated part of the catheter tip, frequency of very early and early shunt failures (revision of the ventricular drainage within 24 hours and within the hospital stay), frequency and percentage of complications (procedure-related and nonsurgical) at discharge.
Discussion: This is the study design of a single center, prospective, randomized controlled trial to investigate whether guided ventriculostomy is superior to the standard freehand technique. One strength of this study is the prospective, randomized, interventional type of study testing a new easy-to-handle guided versus freehand ventricular catheter placement. A second strength of this study is that the power calculation is based on catheter accuracy using an available grading system for catheter tip location, and is calculated with the use of recent study results of our own population, supported by data from prominent studies.
Trial registration: Clinicaltrials.gov identifier: NCT02048553 (registered on 28 January 2014).
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
