

Pathogenesis of nasal polyposis
- PMID: 25482020
- PMCID: PMC4422388
- DOI: 10.1111/cea.12472
Pathogenesis of nasal polyposis
Abstract
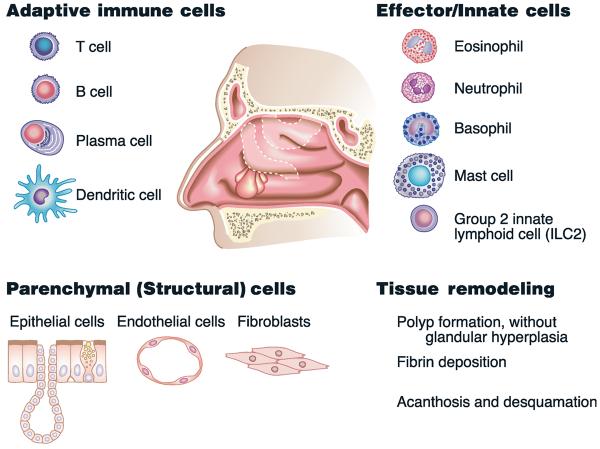
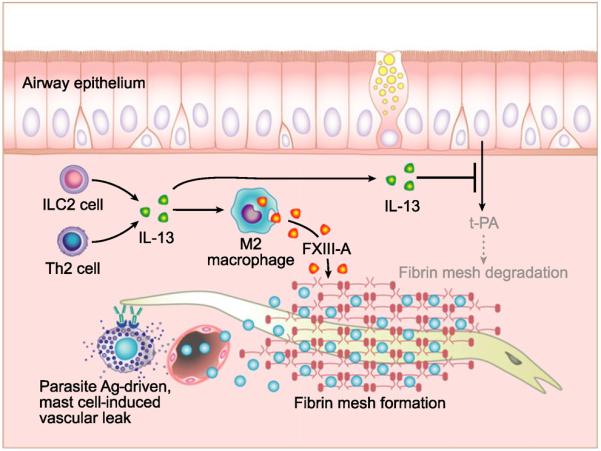
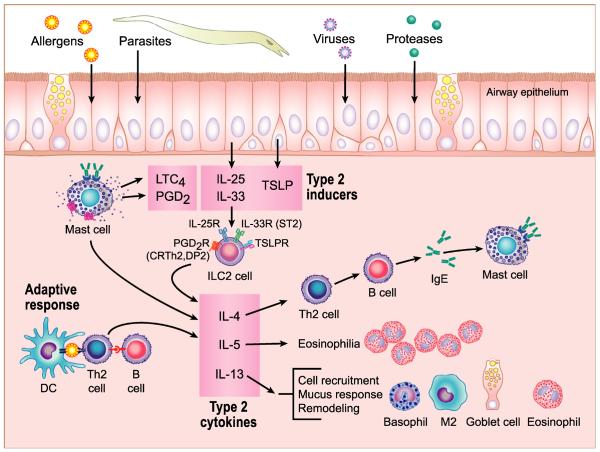
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a complex inflammatory condition that affects a large proportion of the population world-wide and is associated with high cost of management and significant morbidity. Yet, there is a lack of population-based epidemiologic studies using current definitions of CRSwNP, and the mechanisms that drive pathogenesis in this disease remain unclear. In this review, we summarize the current evidence for the plethora of factors that likely contribute to CRSwNP pathogenesis. Defects in the innate function of the airway epithelial barrier, including diminished expression of antimicrobial products and loss of barrier integrity, combined with colonization by fungi and bacteria likely play a critical role in the development of chronic inflammation in CRSwNP. This chronic inflammation is characterized by elevated expression of many key inflammatory cytokines and chemokines, including IL-5, thymic stromal lymphopoietin and CCL11, that help to initiate and perpetuate this chronic inflammatory response. Together, these factors likely combine to drive the influx of a variety of immune cells, including eosinophils, mast cells, group 2 innate lymphoid cells and lymphocytes, which participate in the chronic inflammatory response within the nasal polyps. Importantly, however, future studies are needed to demonstrate the necessity and sufficiency of these potential drivers of disease in CRSwNP. In addition to the development of new tools and models to aid mechanistic studies, the field of CRSwNP research also needs the type of robust epidemiologic data that has served the asthma community so well. Given the high prevalence, costs and morbidity, there is a great need for continued research into CRS that could facilitate the development of novel therapeutic strategies to improve treatment for patients who suffer from this disease.
© 2014 John Wiley & Sons Ltd.
Figures
References
-
- WJ Fokkens, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50:1–12. - PubMed
-
- Jarvis D, Newson R, Lotvall J, et al. Asthma in adults and its association with chronic rhinosinusitis: the GA2LEN survey in Europe. Allergy. 2012;67:91–8. - PubMed
-
- Kim YS, Kim NH, Seong SY, Kim KR, Lee GB, Kim KS. Prevalence and risk factors of chronic rhinosinusitis in Korea. Am J Rhinol Allergy. 2011;25:117–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
