Novel methods for clinical risk stratification in patients with colorectal liver metastases
- PMID: 25483744
- PMCID: PMC4398102
- DOI: 10.4143/crt.2014.066
Novel methods for clinical risk stratification in patients with colorectal liver metastases
Abstract
Purpose: Colorectal cancer patients with liver-confined metastases are classified as stage IV, but their prognoses can differ from metastases at other sites. In this study, we suggest a novel method for risk stratification using clinically effective factors.
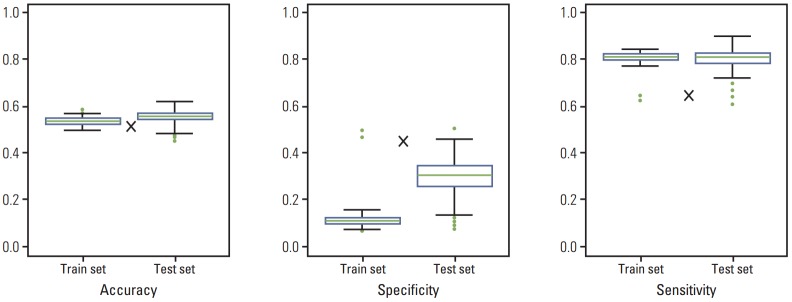
Materials and methods: Data on 566 consecutive patients with colorectal liver metastasis (CLM) between 1989 and 2010 were analyzed. This analysis was based on principal component analysis (PCA).
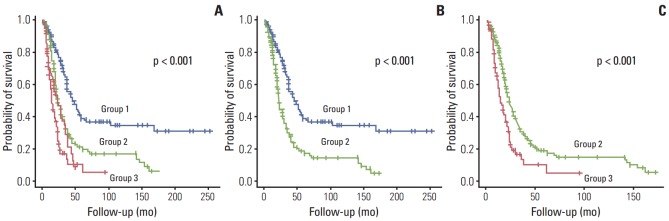
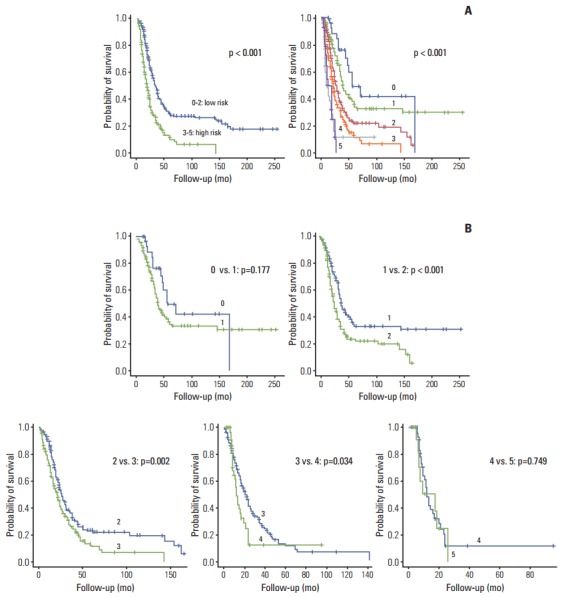
Results: The survival rate was affected by carcinoembryonic antigen (CEA) level (p < 0.001; risk ratio, 1.90), distribution of liver metastasis (p=0.014; risk ratio, 1.46), and disease-free interval (DFI; p < 0.001; risk ratio, 1.98). When patients were divided into three groups according to PCA score using significantly affected factors, they showed significantly different survival patterns (p < 0.001).
Conclusion: The PCA scoring system based on CEA level, distribution of liver metastasis, and DFI may be useful for preoperatively determining prognoses in order to assist in clinical decisionmaking and designing future clinical trials for CLM treatment.
Keywords: Colorectal neoplasms; Liver metastasis; Patient stratification; Risk calculation.
Conflict of interest statement
Conflict of interest relevant to this article was not reported.
Figures
References
-
- Stangl R, Altendorf-Hofmann A, Charnley RM, Scheele J. Factors influencing the natural history of colorectal liver metastases. Lancet. 1994;343:1405–10. - PubMed
-
- Mella J, Biffin A, Radcliffe AG, Stamatakis JD, Steele RJ. Population-based audit of colorectal cancer management in two UK health regions. Colorectal Cancer Working Group, Royal College of Surgeons of England Clinical Epidemiology and Audit Unit. Br J Surg. 1997;84:1731–6. - PubMed
-
- Poston GJ, Adam R, Alberts S, Curley S, Figueras J, Haller D, et al. OncoSurge: a strategy for improving resectability with curative intent in metastatic colorectal cancer. J Clin Oncol. 2005;23:7125–34. - PubMed
-
- Rees M, John TG. Current status of surgery in colorectal metastases to the liver. Hepatogastroenterology. 2001;48:341–4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources