

The Ariadne principles: how to handle multimorbidity in primary care consultations
- PMID: 25484244
- PMCID: PMC4259090
- DOI: 10.1186/s12916-014-0223-1
The Ariadne principles: how to handle multimorbidity in primary care consultations
Abstract
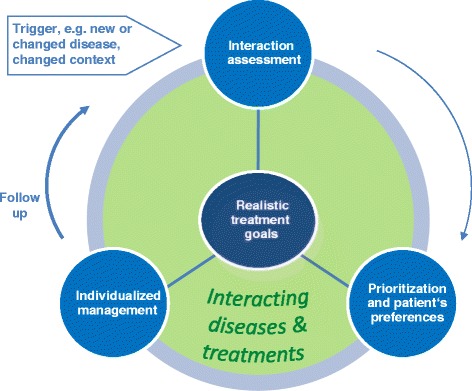
Multimorbidity is a health issue mostly dealt with in primary care practice. As a result of their generalist and patient-centered approach, long-lasting relationships with patients, and responsibility for continuity and coordination of care, family physicians are particularly well placed to manage patients with multimorbidity. However, conflicts arising from the application of multiple disease oriented guidelines and the burden of diseases and treatments often make consultations challenging. To provide orientation in decision making in multimorbidity during primary care consultations, we developed guiding principles and named them after the Greek mythological figure Ariadne. For this purpose, we convened a two-day expert workshop accompanied by an international symposium in October 2012 in Frankfurt, Germany. Against the background of the current state of knowledge presented and discussed at the symposium, 19 experts from North America, Europe, and Australia identified the key issues of concern in the management of multimorbidity in primary care in panel and small group sessions and agreed upon making use of formal and informal consensus methods. The proposed preliminary principles were refined during a multistage feedback process and discussed using a case example. The sharing of realistic treatment goals by physicians and patients is at the core of the Ariadne principles. These result from i) a thorough interaction assessment of the patient's conditions, treatments, constitution, and context; ii) the prioritization of health problems that take into account the patient's preferences - his or her most and least desired outcomes; and iii) individualized management realizes the best options of care in diagnostics, treatment, and prevention to achieve the goals. Goal attainment is followed-up in accordance with a re-assessment in planned visits. The occurrence of new or changed conditions, such as an increase in severity, or a changed context may trigger the (re-)start of the process. Further work is needed on the implementation of the formulated principles, but they were recognized and appreciated as important by family physicians and primary care researchers.Please see related article: http://www.biomedcentral.com/1741-7015/12/222.
Figures

References
-
- van den Akker M, Buntinx F, Knottnerus J. Comorbidity or multimorbidity: what's in a name. A review of literature. Eur J Gen Pract. 1996;2:65–70. doi: 10.3109/13814789609162146. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
