

Steroid unresponsive case of ulcerative mucha-habermann disease (febrile ulcernecrotic mucha-habermann disease) treated with methotrexate
- PMID: 25484416
- PMCID: PMC4248524
- DOI: 10.4103/0019-5154.143572
Steroid unresponsive case of ulcerative mucha-habermann disease (febrile ulcernecrotic mucha-habermann disease) treated with methotrexate
Abstract
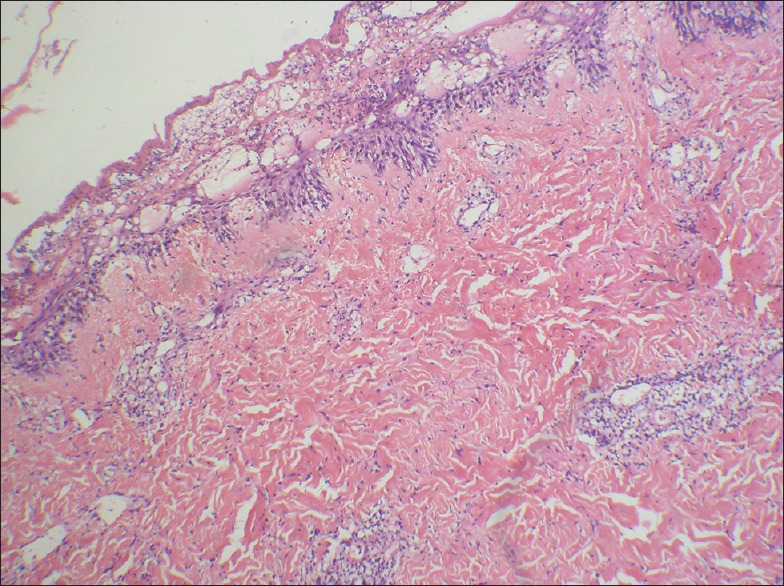
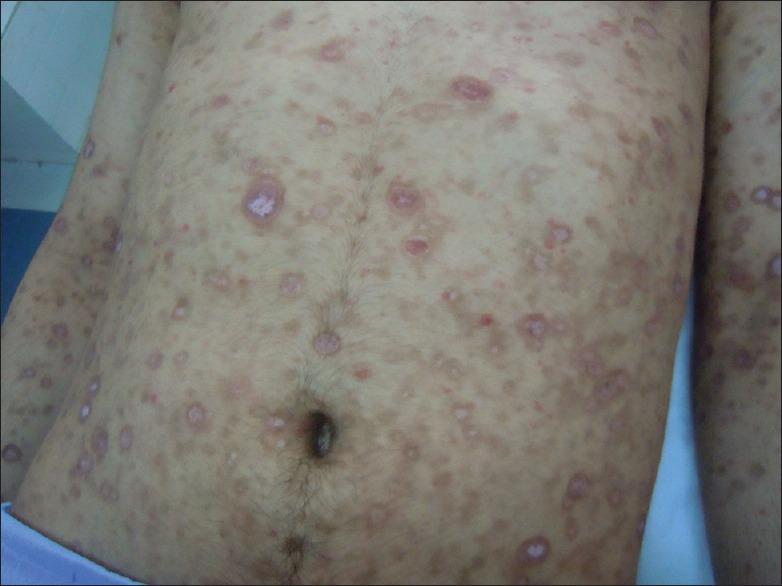
A 20 year old male presented with fever associated with eruption of papules, plaques and vesiculobullous lesions on the chest, back, extremities, palms, soles, and genital mucosa of 20 days duration. Histopathological examination revealed epidermal clefts, edema and vacuolar degeneration of keratinocytes, basal cell degeneration, and dermal perivascular lymphocytic infiltrate. On the basis of clinical features and histology, a diagnosis of febrile ulceronecrotic Mucha-Habermann disease (FUMHD) was made. Treatment with doxycycline (100 mg BD for 4 weeks) and oral prednisolone 60 mg/day tapered to 25 mg in 4 weeks led to initial response that was followed by a relapse on tapering steroid. Addition of methotrexate (7.5 mg increased to 15 mg in 2 weeks) led to a dramatic response.
Keywords: Febrile ulceronecrotic mucha-habermann disease; methotrexate; steroids.
Conflict of interest statement
Figures

Similar articles
-
Febrile ulceronecrotic Mucha-Habermann disease: a case report and review of the literature.Acta Derm Venereol. 2008;88(4):350-5. doi: 10.2340/00015555-0441. Acta Derm Venereol. 2008. PMID: 18709304 Review.
-
A Fatal Case of Febrile Ulceronecrotic Mucha-Habermann Disease which Presenting as Toxic Epidermal Necrolysis.Indian J Dermatol. 2017 Nov-Dec;62(6):675. doi: 10.4103/ijd.IJD_631_16. Indian J Dermatol. 2017. PMID: 29263553 Free PMC article.
-
Febrile ulceronecrotic Mucha-Habermann disease in a 34-month-old boy: a case report and review of the literature.Pediatr Dermatol. 2012 Jan-Feb;29(1):53-8. doi: 10.1111/j.1525-1470.2011.01531.x. Epub 2011 Sep 9. Pediatr Dermatol. 2012. PMID: 21906156 Review.
-
A Diagnostically Challenging Case of Febrile Ulceronecrotic Mucha-Habermann Disease in an Adult Female Successfully Treated with Methotrexate and Cyclosporine.Case Rep Dermatol. 2021 Jan 21;13(1):12-17. doi: 10.1159/000511537. eCollection 2021 Jan-Apr. Case Rep Dermatol. 2021. PMID: 33613228 Free PMC article.
-
Febrile ulceronecrotic Mucha-Habermann disease: a case report and a review of the literature.Dermatol Online J. 2005 Dec 1;11(3):31. Dermatol Online J. 2005. PMID: 16409927 Review.
Cited by
-
Mortality risk factors in febrile ulceronecrotic Mucha- Habermann disease: A systematic review of therapeutic outcomes and complications.Dermatol Reports. 2022 Nov 21;14(4):9492. doi: 10.4081/dr.2022.9492. eCollection 2022 Nov 21. Dermatol Reports. 2022. PMID: 36483219 Free PMC article.
References
-
- Aytekin S, Balci G, Duzgun OY. Febrile ulceronecrotic Mucha-Habermann disease: A case report and a review of the literature. Dermatol Online J. 2005;11:31. - PubMed
-
- Virdi SK, Kanwar AJ, Saikia UN. Pityriasis lichenoides with ulceronecrosis and hyperthermia: A rare variant of pityriasis lichenoides et varioliformis acuta. Indian J Dermatol Venereol Leprol. 2010;76:172–5. - PubMed
-
- Tsai KS, Hsieh HJ, Chow KC, Lin TY, Chiang SF, Huang HH. Detection of cytomegalovirus infection in a patient with febrile ulceronecrotic Mucha-Habermann's disease. Int J Dermatol. 2001;40:694–8. - PubMed
-
- Bowers S, Warshaw EM. Pityriasis lichenoides and its subtypes. J Am Acad Dermatol. 2006;55:557–72. - PubMed
-
- Sotiriou E, Patsatsi A, Tsorova C, Lazaridou E, Sotiriadis D. Febrile ulceronecrotic Mucha-Habermann disease: A case report and review of the literature. Acta Derm Venereol. 2008;88:350–5. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources