

Current concepts in C3 glomerulopathy
- PMID: 25484526
- PMCID: PMC4244712
- DOI: 10.4103/0971-4065.134089
Current concepts in C3 glomerulopathy
Abstract
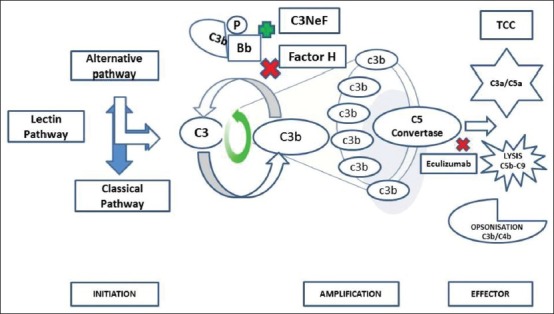
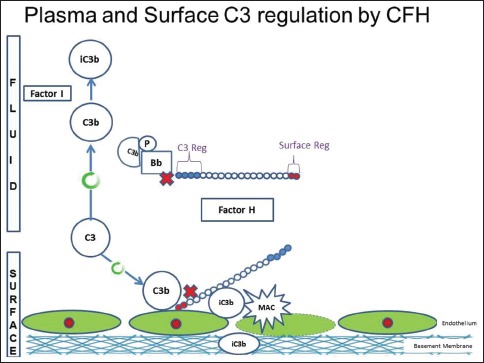
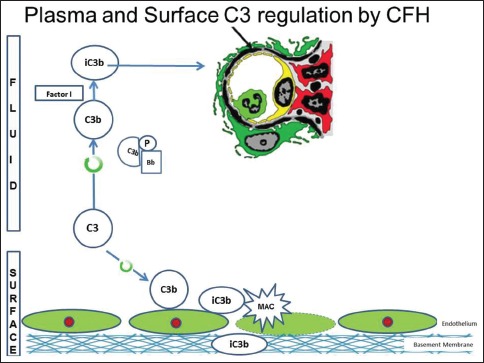
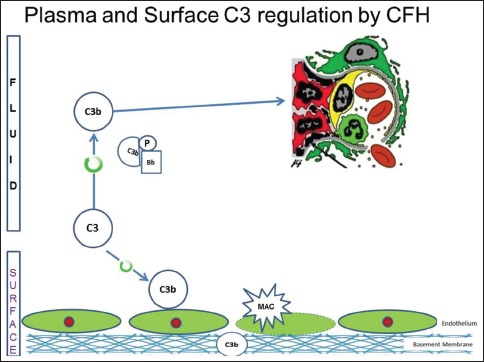
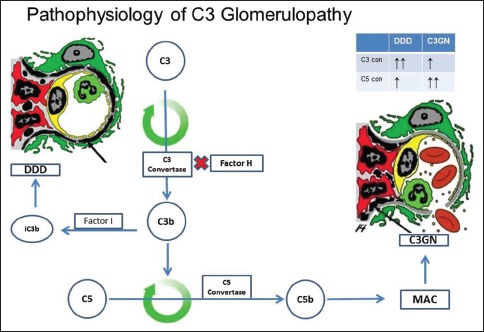
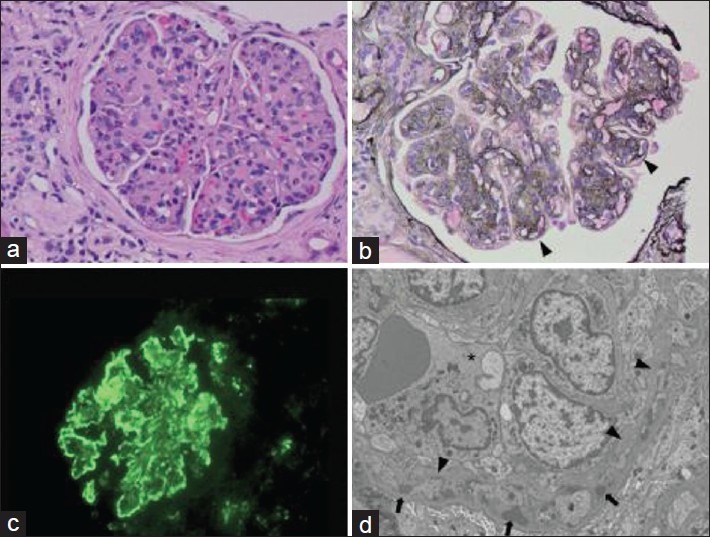
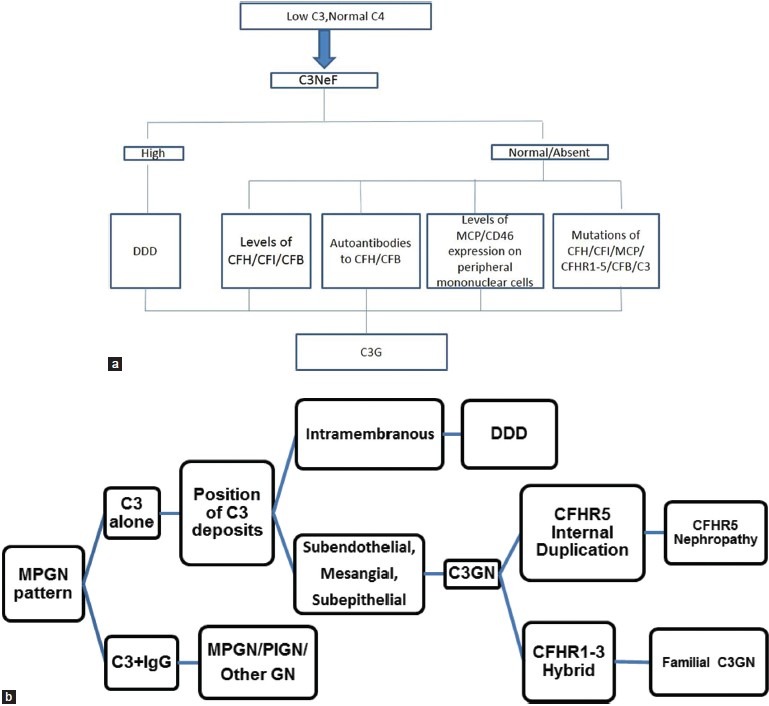
Complement component 3 glomerulopathy (C3G) is a recently defined entity comprising of dense deposit disease and C3 glomerulonephritis. The key histological feature is the presence of isolated C3 deposits without immunoglobulins. Often masqueradng as some of the common glomerulonephritides this is a prototype disorder occurring from dysregulated alternate complement pathway with recently identified genetic defects and autoantibodies. We review the pathophysiology, clinical features, and diagnostic and treatment strategies.
Keywords: Alternate complement pathway; complement component 3 glomerulonephritis; complement component 3 glomerulopathy; complements; dense deposit disease.
Conflict of interest statement
Figures
References
-
- Habib R, Gubler MC, Loirat C, Mäiz HB, Levy M. Dense deposit disease: A variant of membranoproliferative glomerulonephritis. Kidney Int. 1975;7:204–15. - PubMed
-
- Hou J, Markowitz GS, Bomback AS, Appel GB, Herlitz LC, Barry Stokes M, et al. Toward a working definition of C3 glomerulopathy by immunofluorescence. Kidney Int. 2014;85:450–6. - PubMed
-
- Walker PD, Ferrario F, Joh K, Bonsib SM. Dense deposit disease is not a membranoproliferative glomerulonephritis. Mod Pathol. 2007;20:605–16. - PubMed
-
- Gunn WC. The variation in the amount of complement in the blood in some acute infectious diseases and its relation to the clinical features. J Pathol Bacteriol. 1915;19:155–81.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous